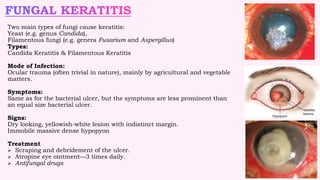
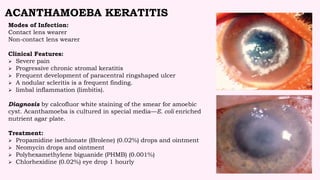
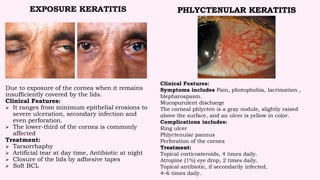
This document summarizes different types of keratitis (inflammation of the cornea). It describes various infectious and non-infectious causes of keratitis including bacteria, viruses, fungi, parasites, exposure, neurotrophic disorders, and hypersensitivity reactions. For each type of keratitis, it outlines the etiology, clinical features such as symptoms and signs, and recommended treatment approaches. The document provides an overview of key information on managing various forms of keratitis for eye care professionals.