Download to read offline

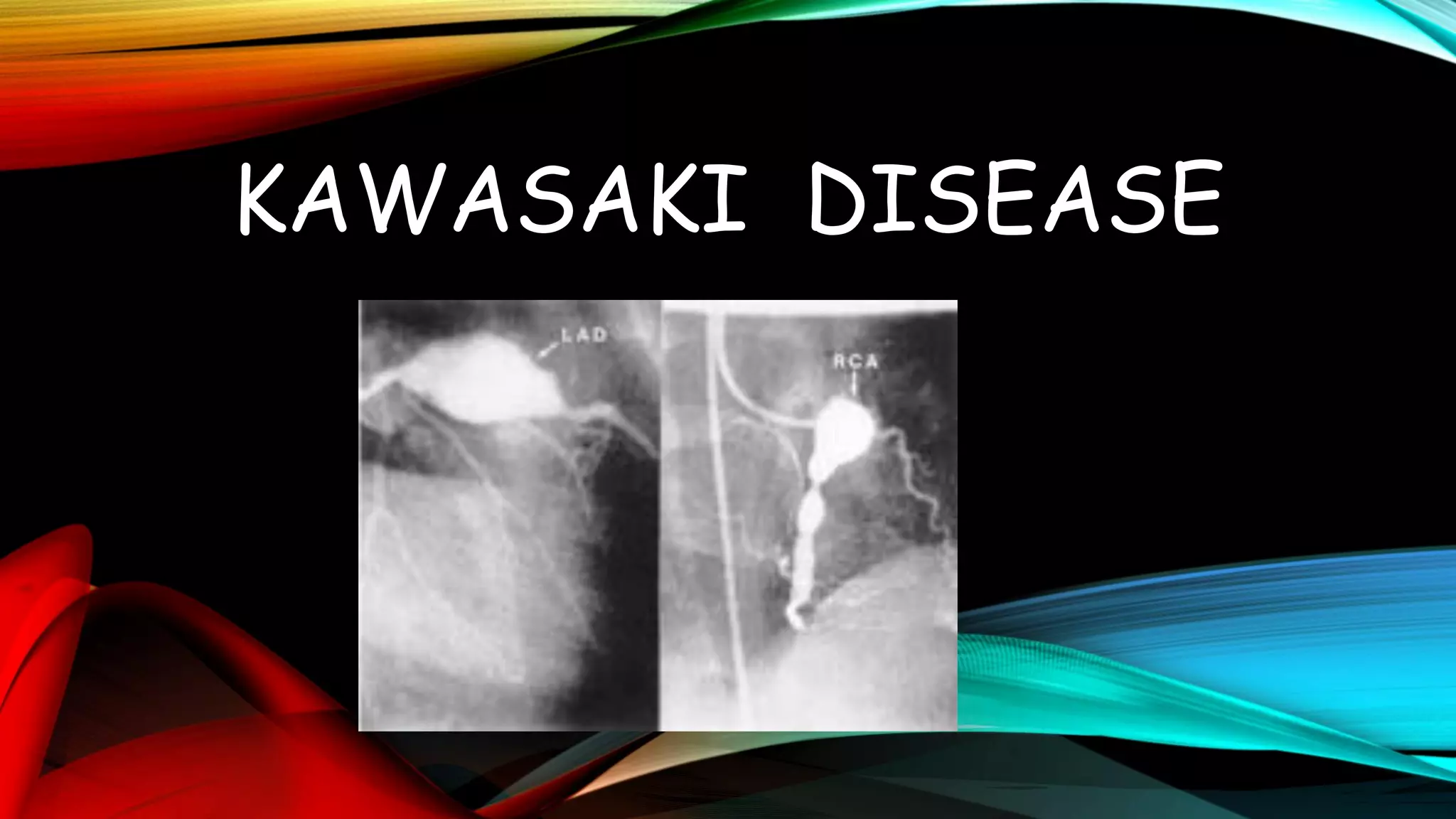

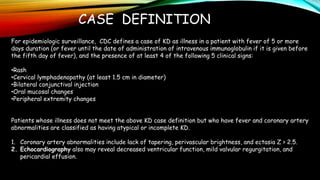
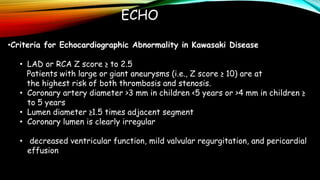
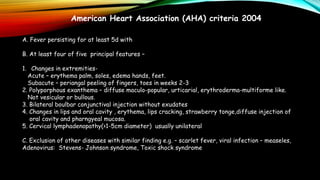
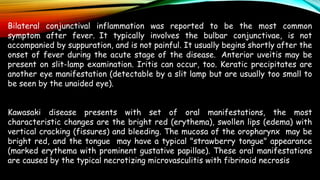
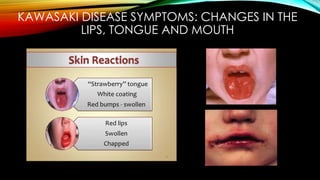
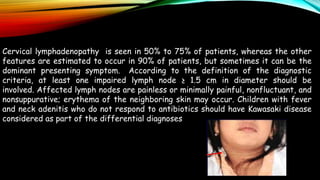

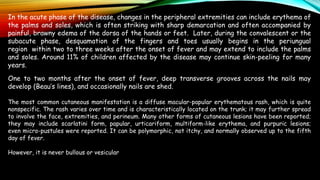
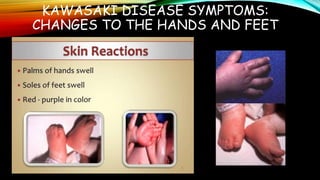





Kawasaki disease is an autoimmune vasculitis that primarily affects children under 5 years old. It is characterized by a high persistent fever and changes in the mouth, hands, feet, skin and eyes including redness of the eyes, red cracked lips, strawberry tongue, and a body rash. If left untreated, it can lead to coronary artery aneurysms in 20-25% of cases which increases the risk of heart attack and death. Treatment involves intravenous immunoglobulin and aspirin to reduce fever and risk of aneurysms developing. Long term risks include coronary artery stenosis and aortic root dilation.







































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















