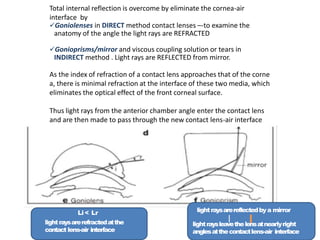
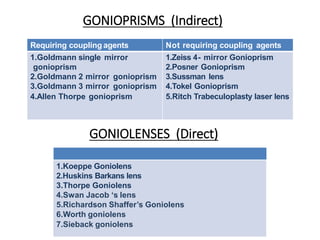
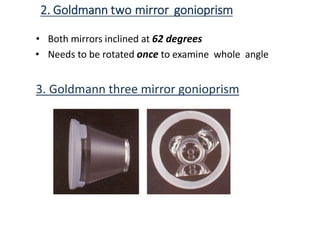
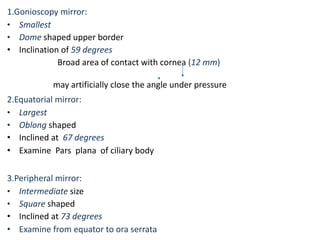
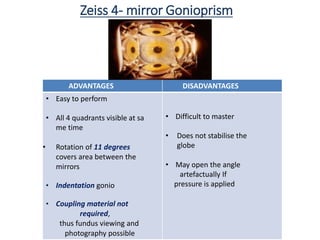
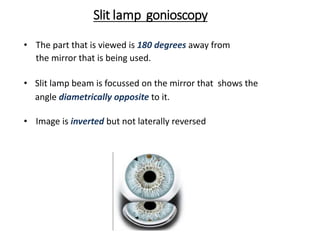
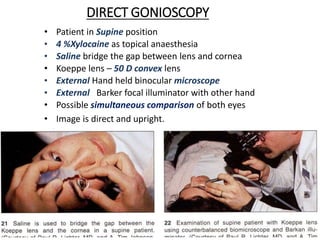
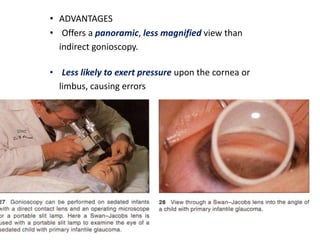
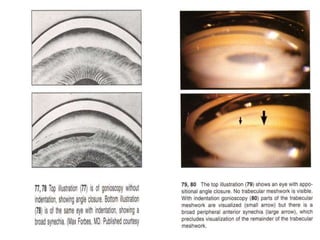
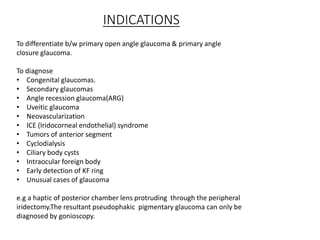
Gonioscopy allows visualization of the anterior chamber angle using contact lenses or prisms to overcome total internal reflection. It can be performed directly using contact lenses like the Koeppe lens or indirectly using prisms like the Goldmann lens. Direct gonioscopy provides an unmagnified panoramic view but requires more equipment while indirect gonioscopy uses a slit lamp for a magnified view but pressure on the cornea can close the angle. Both methods allow assessment of the angle and detection of pathologies.