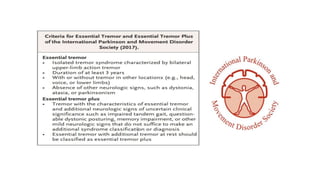
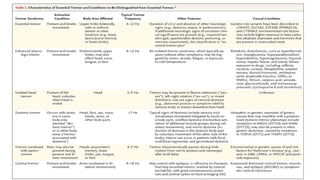
1) Essential tremor is a syndrome of isolated tremor of the upper limbs that has been present for at least 3 years, with or without tremor in other locations like the head or voice.
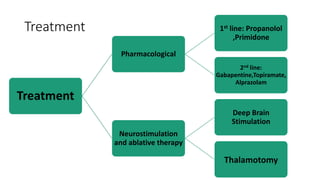
2) Propranolol and primidone are first-line pharmacological treatments that can reduce tremor severity by 55-60% through effects on the cortico-ponto-cerebellar-thalamic circuit implicated in essential tremor pathophysiology.
3) When medications are ineffective, neurostimulation techniques like deep brain stimulation targeting the thalamus or focused ultrasound thalamotomy can provide relief of tremors, though effectiveness may diminish over time and risks include ataxia, dys