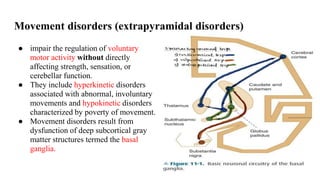
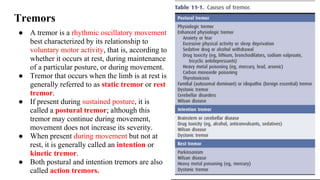
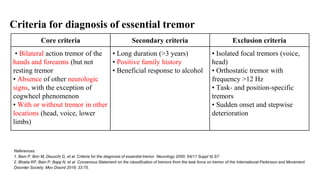
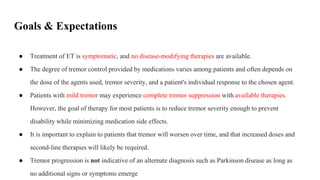
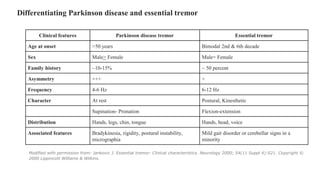
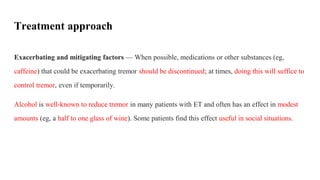
Movement disorders, particularly essential tremors, impair voluntary motor activity due to basal ganglia dysfunction, leading to involuntary movements. Essential tremor is the most common cause of action tremor in adults, often requiring symptomatic treatment to manage tremor severity and prevent disability. Diagnosis criteria include bilateral action tremor and family history, with treatment options ranging from beta blockers and anti-seizure medications to adaptive devices and botulinum toxin injections.


![Cont..
● Alprazolam may be useful for the treatment of limb tremor associated with ET in select patients,
although high-quality data are lacking. Two small clinical trials found that alprazolam, 0.125 to
3 mg/day, was associated with an improvement in clinical rating scales of 25 to 34 percent
compared with placebo. Side effects included mild sedation and fatigue. A tremor reduction of
69 and 76 percent (according to electromyography [EMG] data recorded at 40 and 80 minutes,
respectively, after a dose of alprazolam) was documented in a study involving eight patients.
● Clonazepam is occasionally used for the treatment of limb tremor associated with ET, although
data are mixed. One clinical trial found that clonazepam 0.5 to 6 mg/day significantly reduced
tremor, while another study found that clonazepam 0.4 to 4 mg/day was ineffective and resulted](https://image.slidesharecdn.com/essentialtremors-240728110423-f4448fba/85/Essential-Tremors-Movement-Disorder-pptx-23-320.jpg)