Ommen, S.R. etal, 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic
Cardiomyopathy. Circulation.
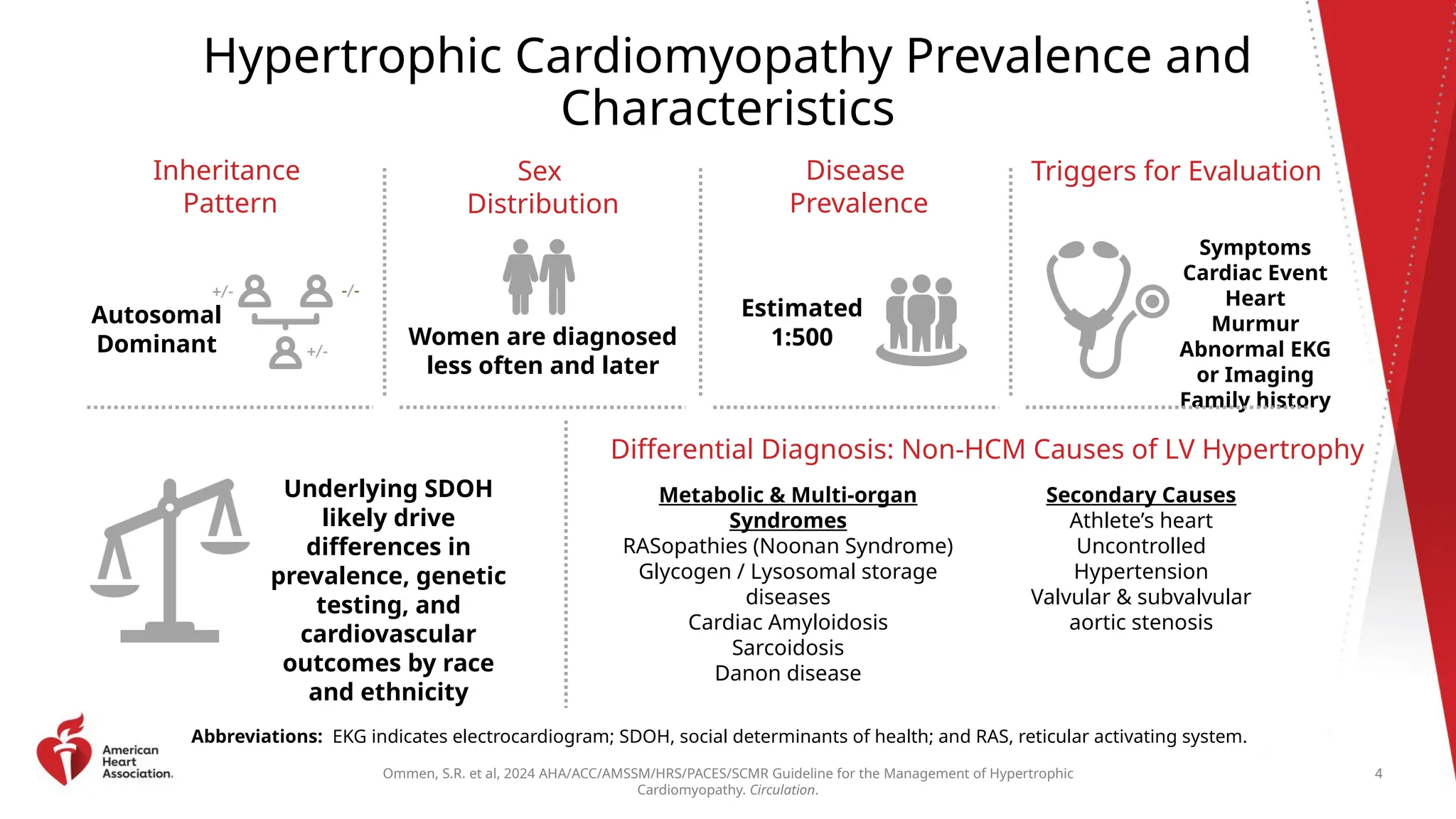
Hypertrophic Cardiomyopathy Prevalence and
Characteristics
Inheritance
Pattern
Autosomal
Dominant
Sex
Distribution
Women are diagnosed
less often and later
Disease
Prevalence
Estimated
1:500
Triggers for Evaluation
Symptoms
Cardiac Event
Heart
Murmur
Abnormal EKG
or Imaging
Family history
Underlying SDOH
likely drive
differences in
prevalence, genetic
testing, and
cardiovascular
outcomes by race
and ethnicity
Differential Diagnosis: Non-HCM Causes of LV Hypertrophy
Metabolic & Multi-organ
Syndromes
RASopathies (Noonan Syndrome)
Glycogen / Lysosomal storage
diseases
Cardiac Amyloidosis
Sarcoidosis
Danon disease
Secondary Causes
Athlete’s heart
Uncontrolled
Hypertension
Valvular & subvalvular
aortic stenosis
Abbreviations: EKG indicates electrocardiogram; SDOH, social determinants of health; and RAS, reticular activating system.
4
+/- -/-
+/-
5.
Ommen, S.R. etal, 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic
Cardiomyopathy. Circulation.
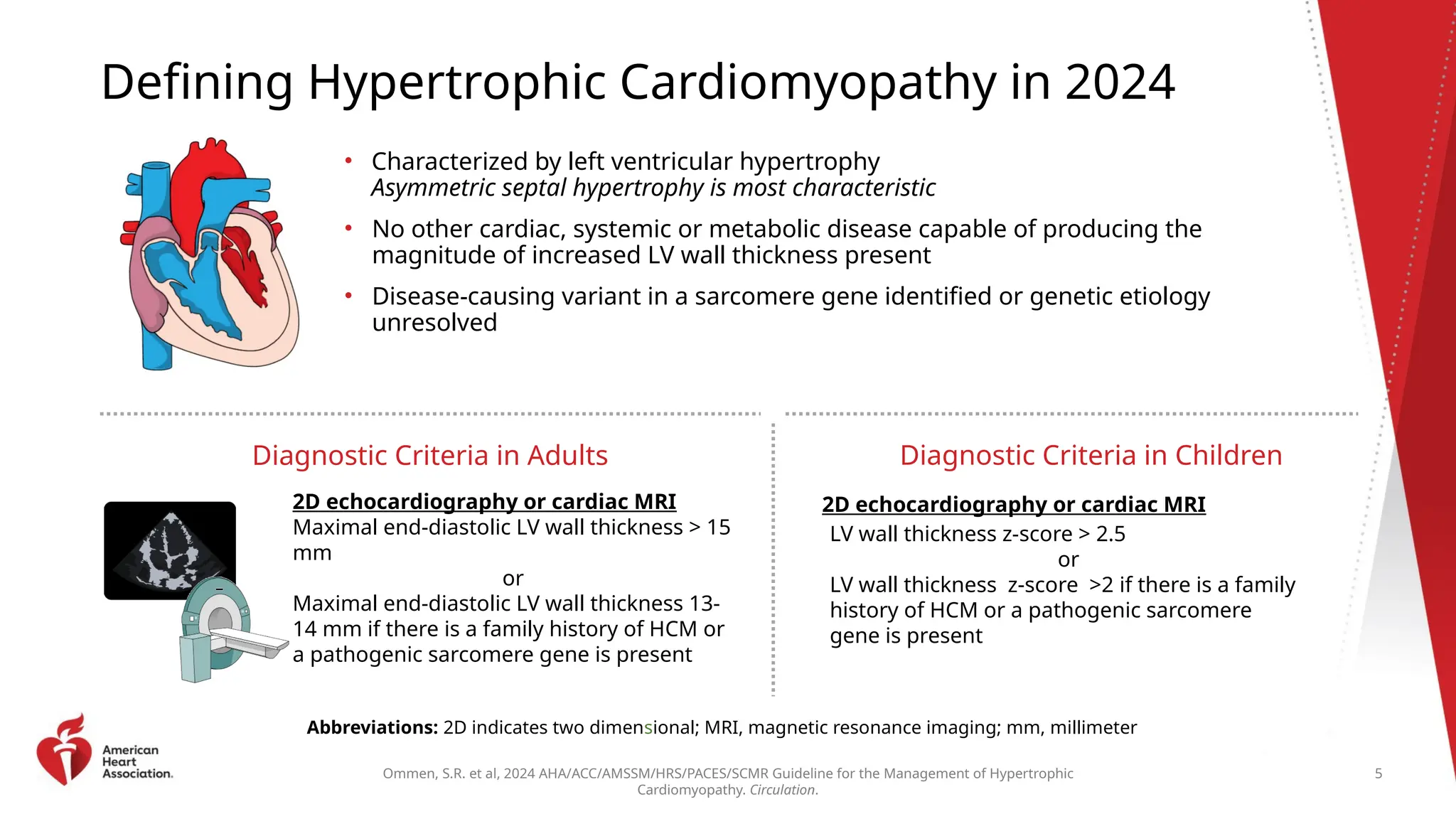
Defining Hypertrophic Cardiomyopathy in 2024
• Characterized by left ventricular hypertrophy
Asymmetric septal hypertrophy is most characteristic
• No other cardiac, systemic or metabolic disease capable of producing the
magnitude of increased LV wall thickness present
• Disease-causing variant in a sarcomere gene identified or genetic etiology
unresolved
Diagnostic Criteria in Adults
2D echocardiography or cardiac MRI
Maximal end-diastolic LV wall thickness > 15
mm
or
Maximal end-diastolic LV wall thickness 13-
14 mm if there is a family history of HCM or
a pathogenic sarcomere gene is present
Diagnostic Criteria in Children
Abbreviations: 2D indicates two dimensional; MRI, magnetic resonance imaging; mm, millimeter
5
LV wall thickness z-score > 2.5
or
LV wall thickness z-score >2 if there is a family
history of HCM or a pathogenic sarcomere
gene is present
2D echocardiography or cardiac MRI
Ommen, S.R. etal, 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic
Cardiomyopathy. Circulation.
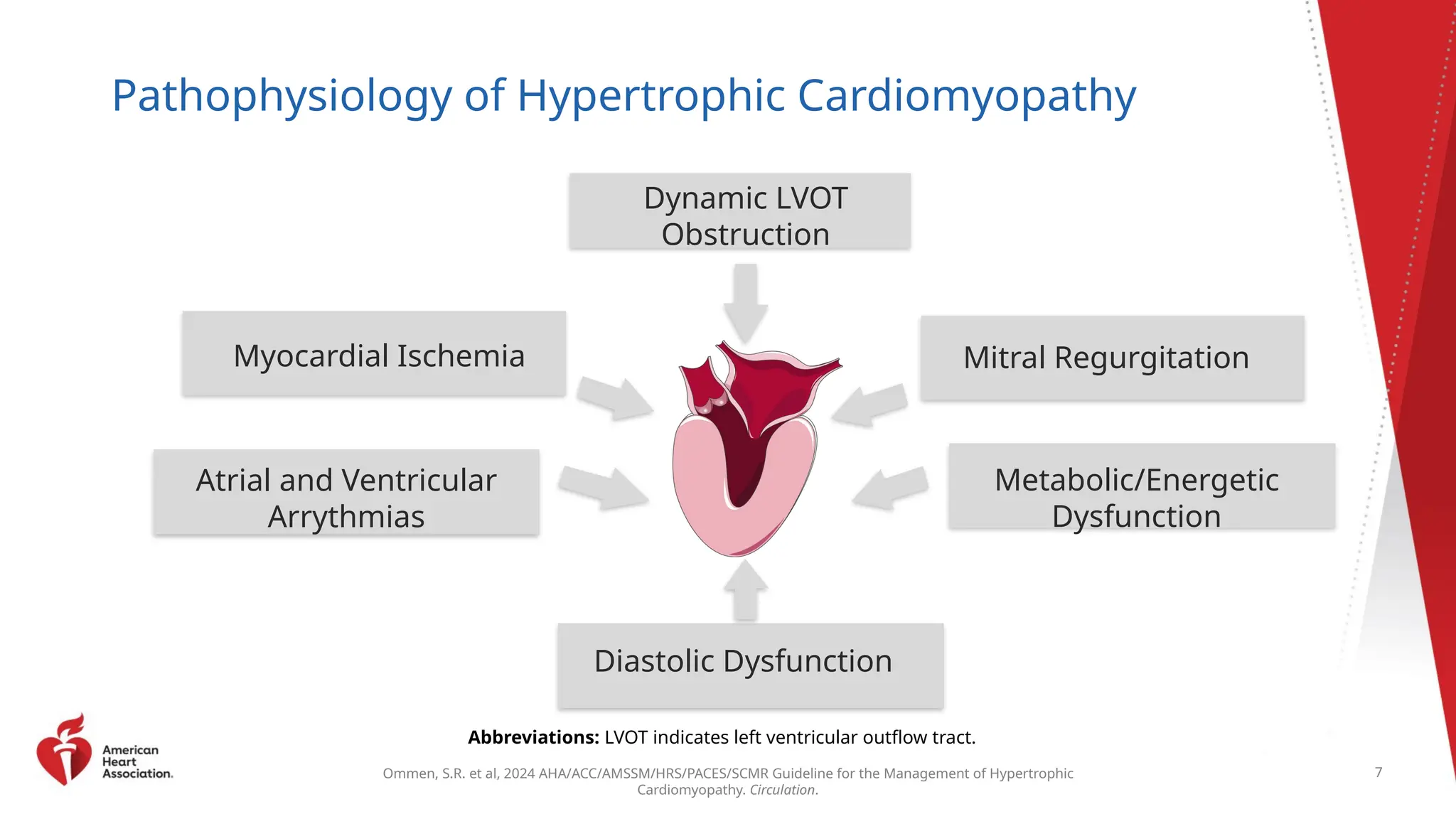
Pathophysiology of Hypertrophic Cardiomyopathy
Dynamic LVOT
Obstruction
Mitral Regurgitation
Metabolic/Energetic
Dysfunction
Diastolic Dysfunction
Myocardial Ischemia
Abbreviations: LVOT indicates left ventricular outflow tract.
7
Atrial and Ventricular
Arrythmias
8.
Ommen, S.R. etal, 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic
Cardiomyopathy. Circulation.
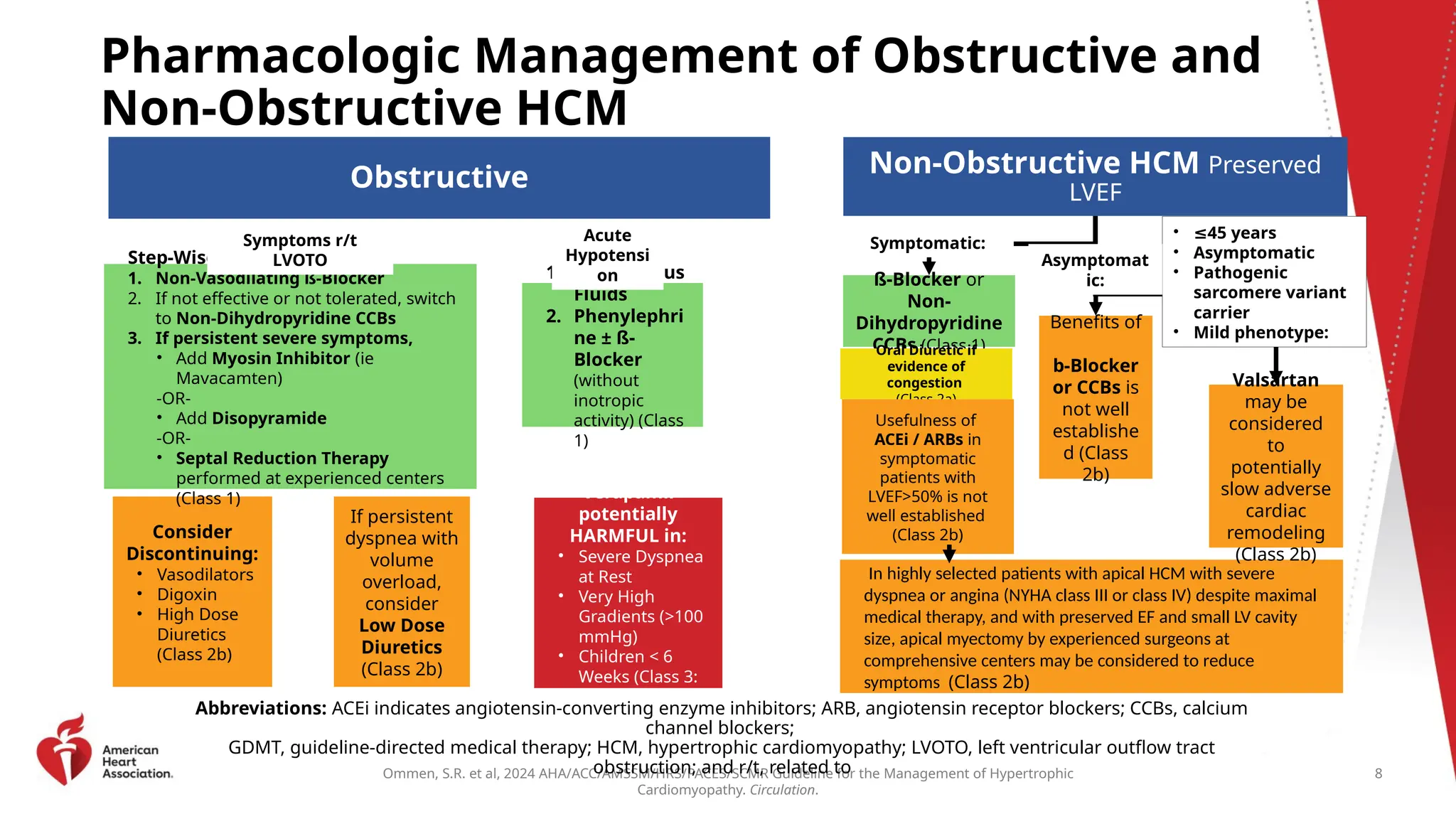
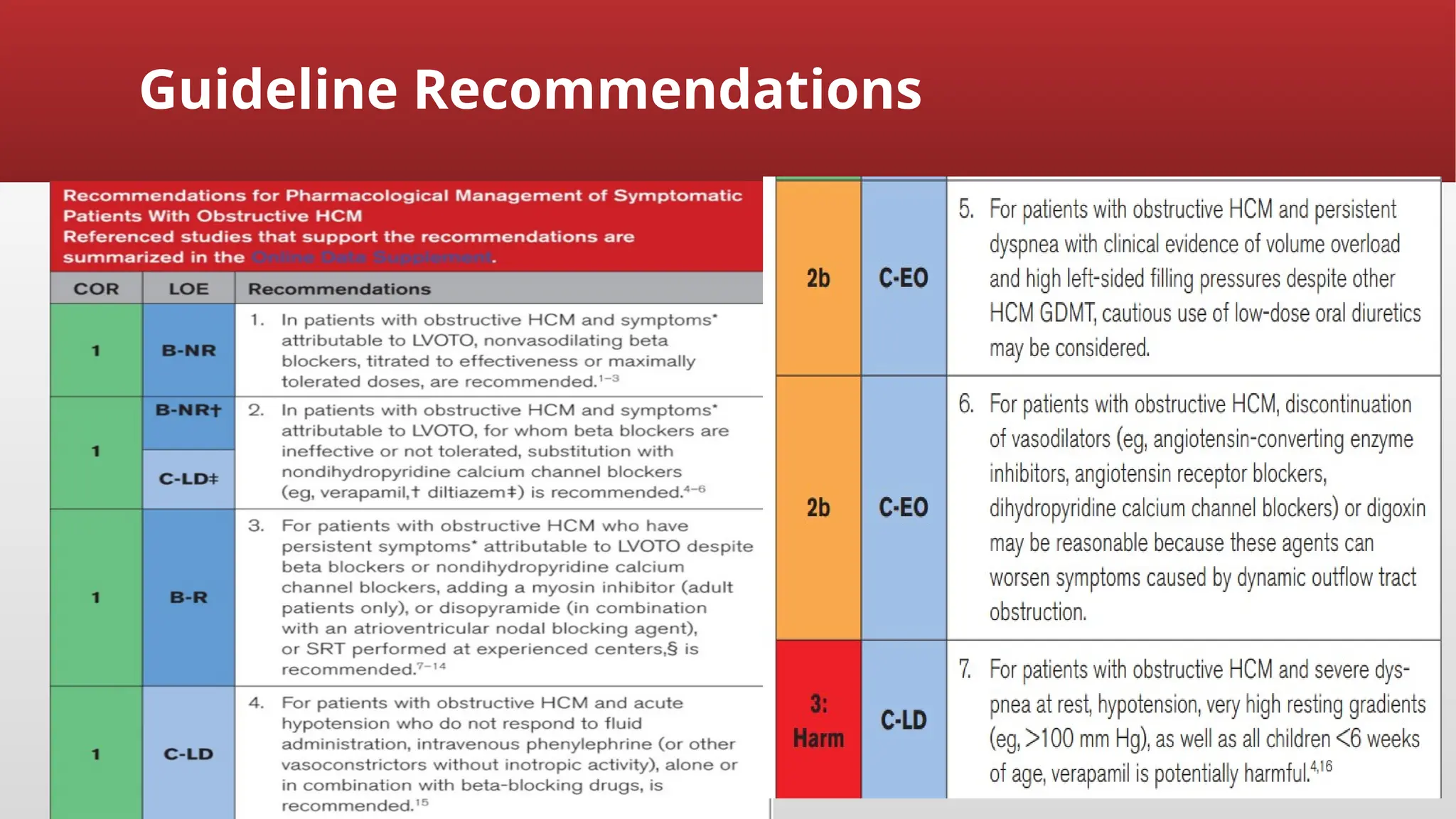
Pharmacologic Management of Obstructive and
Non-Obstructive HCM
Abbreviations: ACEi indicates angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; CCBs, calcium
channel blockers;
GDMT, guideline-directed medical therapy; HCM, hypertrophic cardiomyopathy; LVOTO, left ventricular outflow tract
obstruction; and r/t, related to
Obstructive
If persistent
dyspnea with
volume
overload,
consider
Low Dose
Diuretics
(Class 2b)
Non-Obstructive HCM Preserved
LVEF
In highly selected patients with apical HCM with severe
dyspnea or angina (NYHA class III or class IV) despite maximal
medical therapy, and with preserved EF and small LV cavity
size, apical myectomy by experienced surgeons at
comprehensive centers may be considered to reduce
symptoms (Class 2b)
Consider
Discontinuing:
• Vasodilators
• Digoxin
• High Dose
Diuretics
(Class 2b)
Verapamil
potentially
HARMFUL in:
• Severe Dyspnea
at Rest
• Very High
Gradients (>100
mmHg)
• Children < 6
Weeks (Class 3:
Harm)
1. Intravenous
Fluids
2. Phenylephri
ne ± ß-
Blocker
(without
inotropic
activity) (Class
1)
Step-Wise Approach:
1. Non-Vasodilating ß-Blocker
2. If not effective or not tolerated, switch
to Non-Dihydropyridine CCBs
3. If persistent severe symptoms,
• Add Myosin Inhibitor (ie
Mavacamten)
-OR-
• Add Disopyramide
-OR-
• Septal Reduction Therapy
performed at experienced centers
(Class 1)
ß-Blocker or
Non-
Dihydropyridine
CCBs (Class 1)
Oral Diuretic if
evidence of
congestion
(Class 2a)
Benefits of
b-Blocker
or CCBs is
not well
establishe
d (Class
2b)
Valsartan
may be
considered
to
potentially
slow adverse
cardiac
remodeling
(Class 2b)
Usefulness of
ACEi / ARBs in
symptomatic
patients with
LVEF>50% is not
well established
(Class 2b)
• ≤45 years
• Asymptomatic
• Pathogenic
sarcomere variant
carrier
• Mild phenotype:
Symptomatic:
Asymptomat
ic:
8
Symptoms r/t
LVOTO
Acute
Hypotensi
on
9.
Ommen, S.R. etal, 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic
Cardiomyopathy. Circulation.
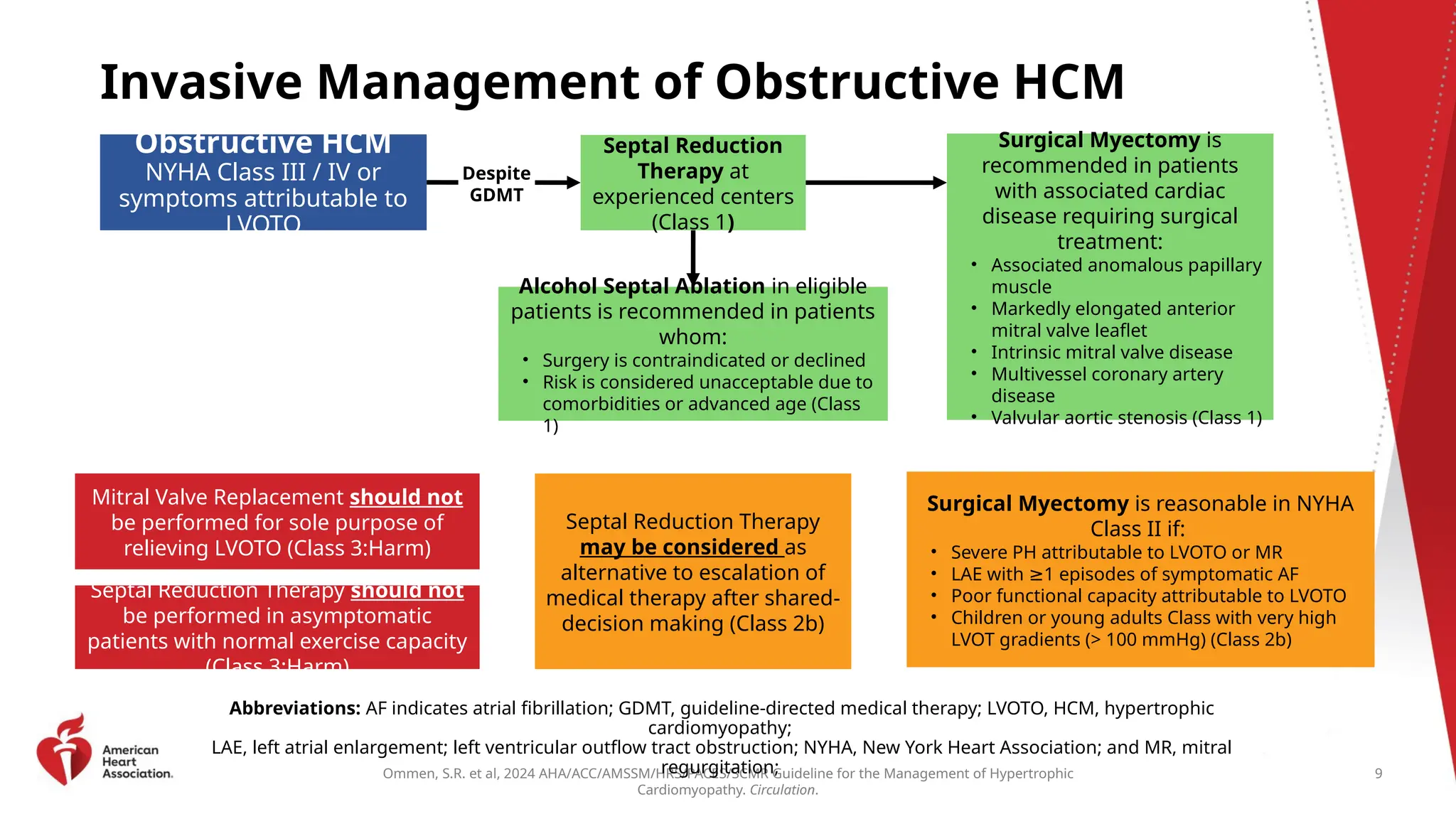
Invasive Management of Obstructive HCM
Abbreviations: AF indicates atrial fibrillation; GDMT, guideline-directed medical therapy; LVOTO, HCM, hypertrophic
cardiomyopathy;
LAE, left atrial enlargement; left ventricular outflow tract obstruction; NYHA, New York Heart Association; and MR, mitral
regurgitation;
Obstructive HCM
NYHA Class III / IV or
symptoms attributable to
LVOTO
Septal Reduction
Therapy at
experienced centers
(Class 1)
Despite
GDMT
Alcohol Septal Ablation in eligible
patients is recommended in patients
whom:
• Surgery is contraindicated or declined
• Risk is considered unacceptable due to
comorbidities or advanced age (Class
1)
Surgical Myectomy is
recommended in patients
with associated cardiac
disease requiring surgical
treatment:
• Associated anomalous papillary
muscle
• Markedly elongated anterior
mitral valve leaflet
• Intrinsic mitral valve disease
• Multivessel coronary artery
disease
• Valvular aortic stenosis (Class 1)
Mitral Valve Replacement should not
be performed for sole purpose of
relieving LVOTO (Class 3:Harm)
Septal Reduction Therapy should not
be performed in asymptomatic
patients with normal exercise capacity
(Class 3:Harm)
Septal Reduction Therapy
may be considered as
alternative to escalation of
medical therapy after shared-
decision making (Class 2b)
Surgical Myectomy is reasonable in NYHA
Class II if:
• Severe PH attributable to LVOTO or MR
• LAE with 1 episodes of symptomatic AF
≥
• Poor functional capacity attributable to LVOTO
• Children or young adults Class with very high
LVOT gradients (> 100 mmHg) (Class 2b)
9
10.
Weekly Journal Club;MAPLE-HCM Trial 10
cont'd...
Beta-blockers have been the initial treatment for symptomatic obstructive hypertrophic
cardiomyopathy (oHCM) despite limited evidence of their efficacy.
Aficamten is a cardiac myosin inhibitor(CMI)
reduces left ventricular outflow tract gradients,
improves exercise capacity, and
decreases HCM symptoms when added to standard medications.
19/09/2025
Weekly Journal Club;MAPLE-HCM Trial 18
objective
the over all objectives of this head to head comparison trial is to evaluate the safety and
efficacy of aficamten as:
first line therapy for participants recently diagnosed with symptomatic oHCM and/or
treatment naive: or
monotherapy for participants previously receiving standard of care(SOC) medical therapy
for symptomatic oHCM.
19/09/2025
Weekly Journal Club;MAPLE-HCM Trial 20
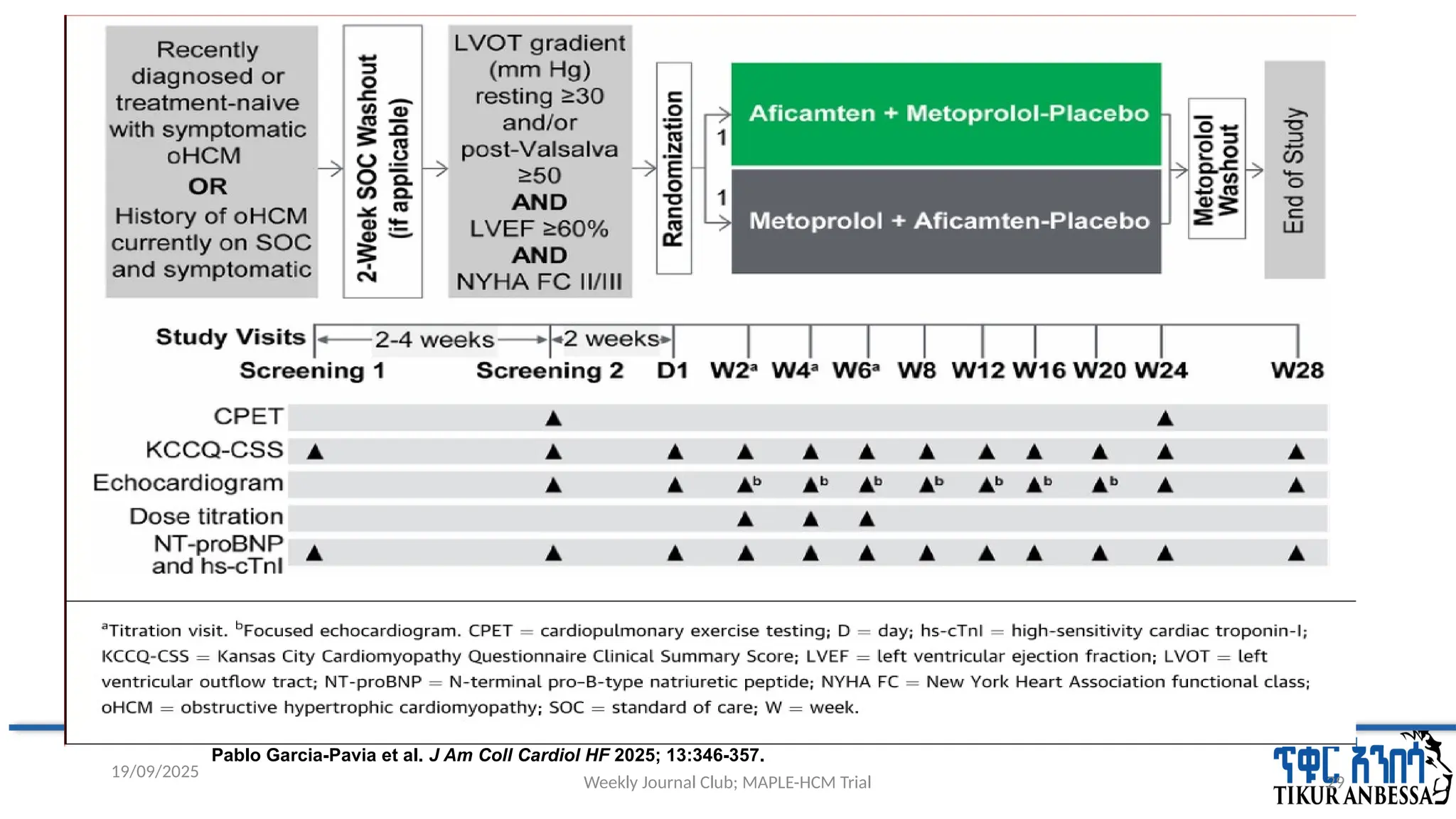
Methodology
trial design
multicenter, randomized ,international, double-blind, double-dummy, a head-to-head,
phase 3 trial
study was conducted from June 2023, to August 2024, across 71 sites
in North America, Brazil, Europe, Israel, and China;
19/09/2025
21.
Weekly Journal Club;MAPLE-HCM Trial 21
Ethical clearance and funding
the trial was conducted in accordance with the principles of the Declaration of Helsinki and the
International Council for Harmonisation Good Clinical Practice guidelines.
An academic steering committee in collaboration with Cytokinetics (the sponsor)
designed the trial,
selected clinical trial centers,
oversaw the conduct and monitoring of the trial
All the patients provided written informed consent.
19/09/2025
Weekly Journal Club;MAPLE-HCM Trial 24
Procedure
Patients underwent randomization within 6 weeks after the start of screening.
patients underwent a washout of background standard therapy of up to 2 weeks beginning
at the first screening visit.
patients reduced the dose of standard medications every 2 days until standard
medications were discontinued for at least 7 days before screening assessments.
19/09/2025
25.
Weekly Journal Club;MAPLE-HCM Trial 25
cont'd...
To understand whether current or recent use of standard medications or time since HCM diagnosis
influenced the effect of treatment, patients were divided into two groups:
group 1 included patients who had recently (≤12 months) received a diagnosis of HCM or had not
received standard medications in the past 12 months, regardless of the date of diagnosis;
group 2 included patients with a long-standing (>12 months) HCM diagnosis who had received
standard medications within the past 12 months.
19/09/2025
26.
Weekly Journal Club;MAPLE-HCM Trial 26
cont'd...
Enrollment of patients who had previously received mavacamten and those who had undergone
septal reduction therapy was capped at approximately 10% each,
Enrollment of patients who used a cycle ergometer for exercise testing was capped at
approximately 50%.
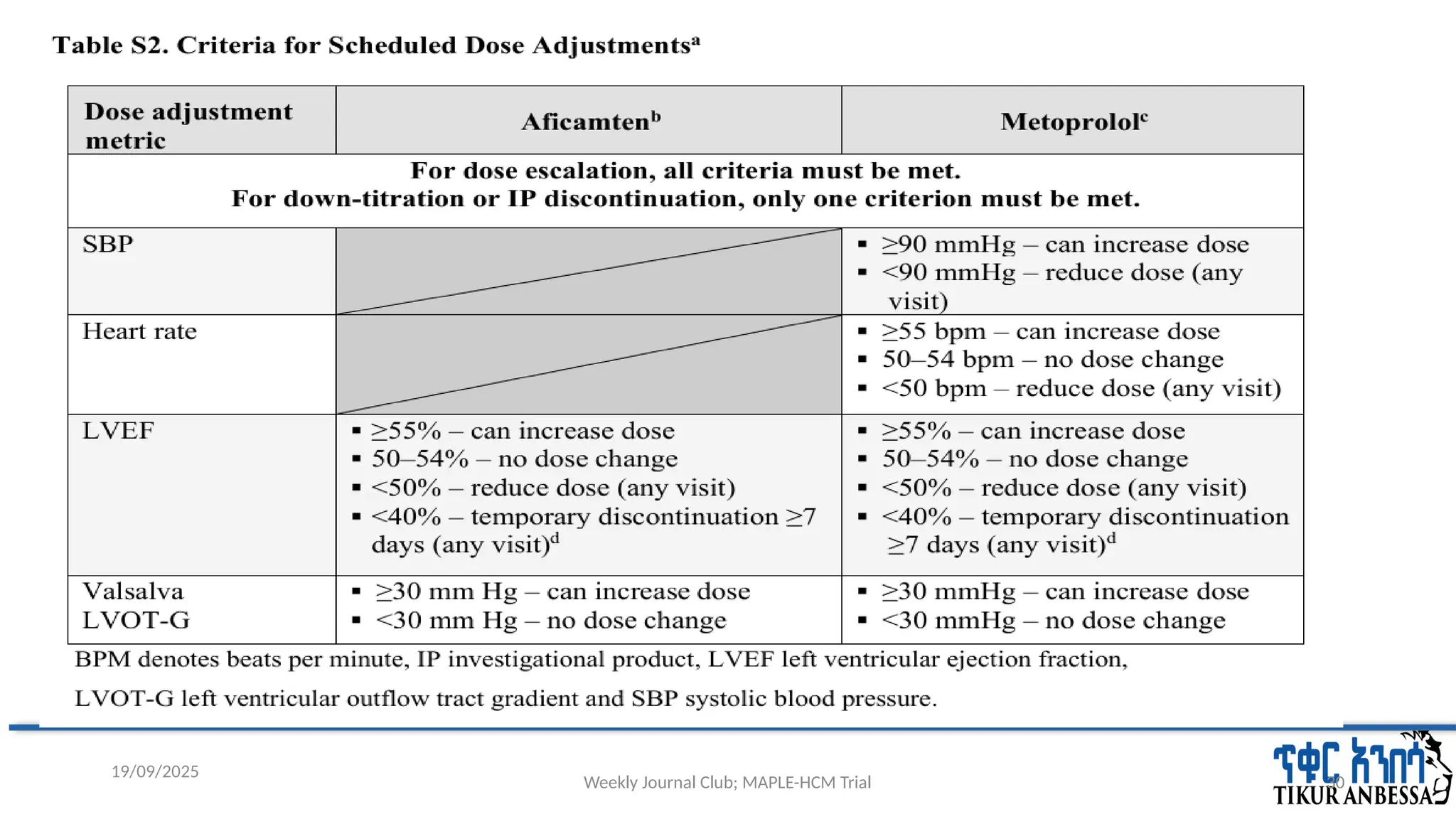
The starting dose of aficamten was 5 mg and of metoprolol was 50 mg.
At weeks 2, 4, and 6, the dose of aficamten could be escalated in 5-mg increments and the dose of
metoprolol could be escalated in 50-mg increments, to a maximum dose of 20 mg and 200 mg,
respectively.
19/09/2025
27.
Weekly Journal Club;MAPLE-HCM Trial 27
Statistical Analysis
The statistical power for the primary end point was calculated under the assumption that the
difference between groups in the change in peak oxygen uptake at week 24 would be
2ml/kg/minute, with a standard deviation of 3ml/kg/minute.
With the estimated sample size of 170 patients would provide the trial with more than 90% power
to detect a difference in peak oxygen uptake at a two-sided type I error level of 0.05.
The primary end point was analyzed with the use of an analysis of covariance model, with
treatment group, randomization stratification factors, baseline peak oxygen uptake.
19/09/2025
28.
Weekly Journal Club;MAPLE-HCM Trial 28
cont'd...
Other secondary end points were analyzed with the use of a mixed model for repeated measures.
Safety analyses were performed in the safety analysis population, which included all the patients
who received at least one dose of aficamten or metoprolol.
For all subgroup analyses, the widths of the 95% confidence intervals have not been adjusted for
multiplicity and the intervals should not be used in place of hypothesis testing.
19/09/2025
29.
Weekly Journal Club;MAPLE-HCM Trial 29
19/09/2025
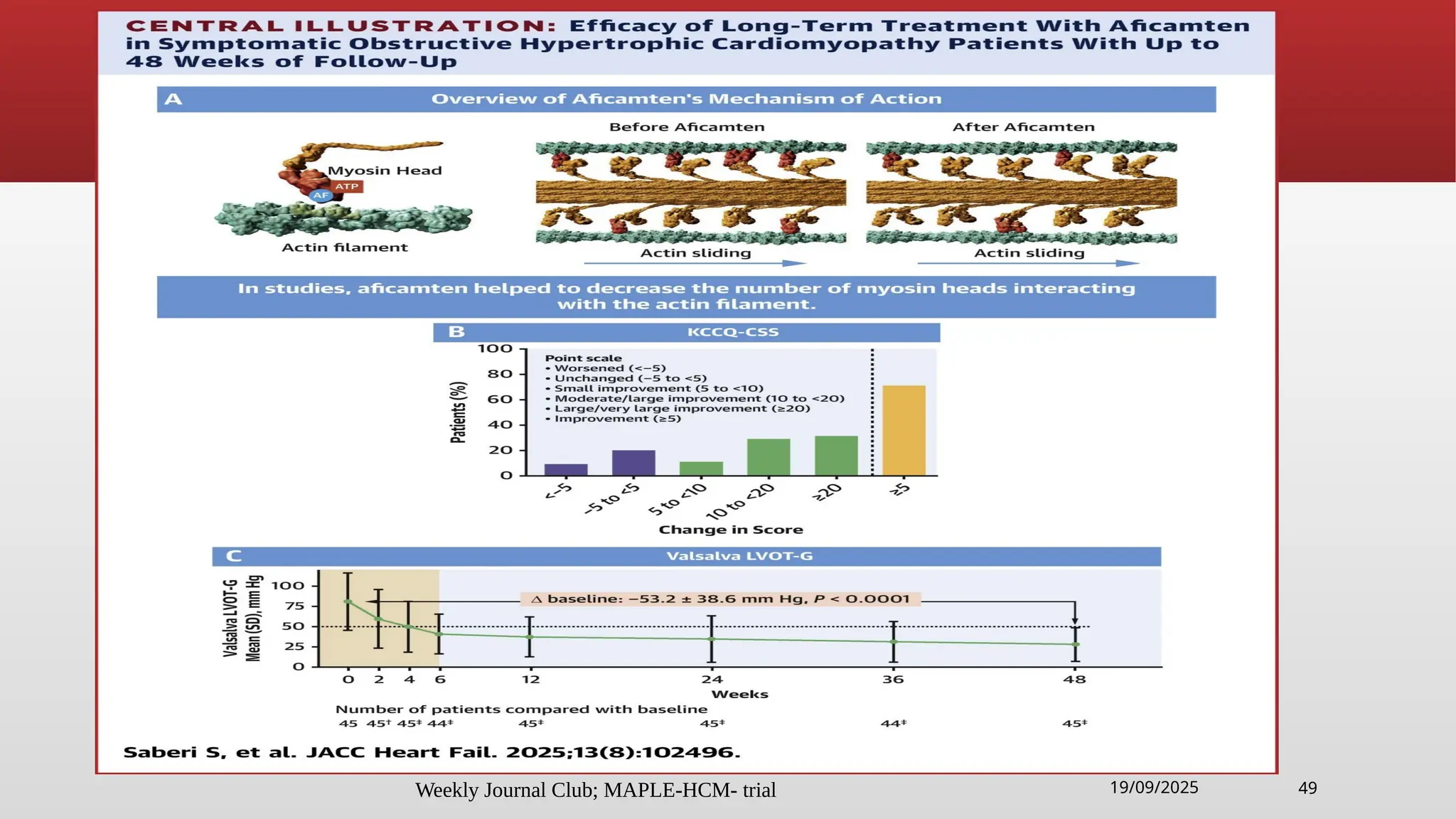
Pablo Garcia-Pavia et al. J Am Coll Cardiol HF 2025; 13:346-357.
Weekly Journal Club;MAPLE-HCM Trial 35
cont'd...
At week 24, in the aficamten group a total of :
66 (76%) were receiving 15mg or 20mg of aficamten
the dose decreased to 0 mg for 1 patient (1%) owing to unacceptable side effects at the
lowest dose, in accordance with the dose-adjustment algorithm.
In comparison, in the metoprolol group:
53(63%) were receiving 150mg or 200mg of metoprolol
the dose decreased to 0 mg for 10 patients (12%) owing to unacceptable side effects at the
lowest dose.
19/09/2025
Weekly Journal Club;MAPLE-HCM Trial 45
Discussion
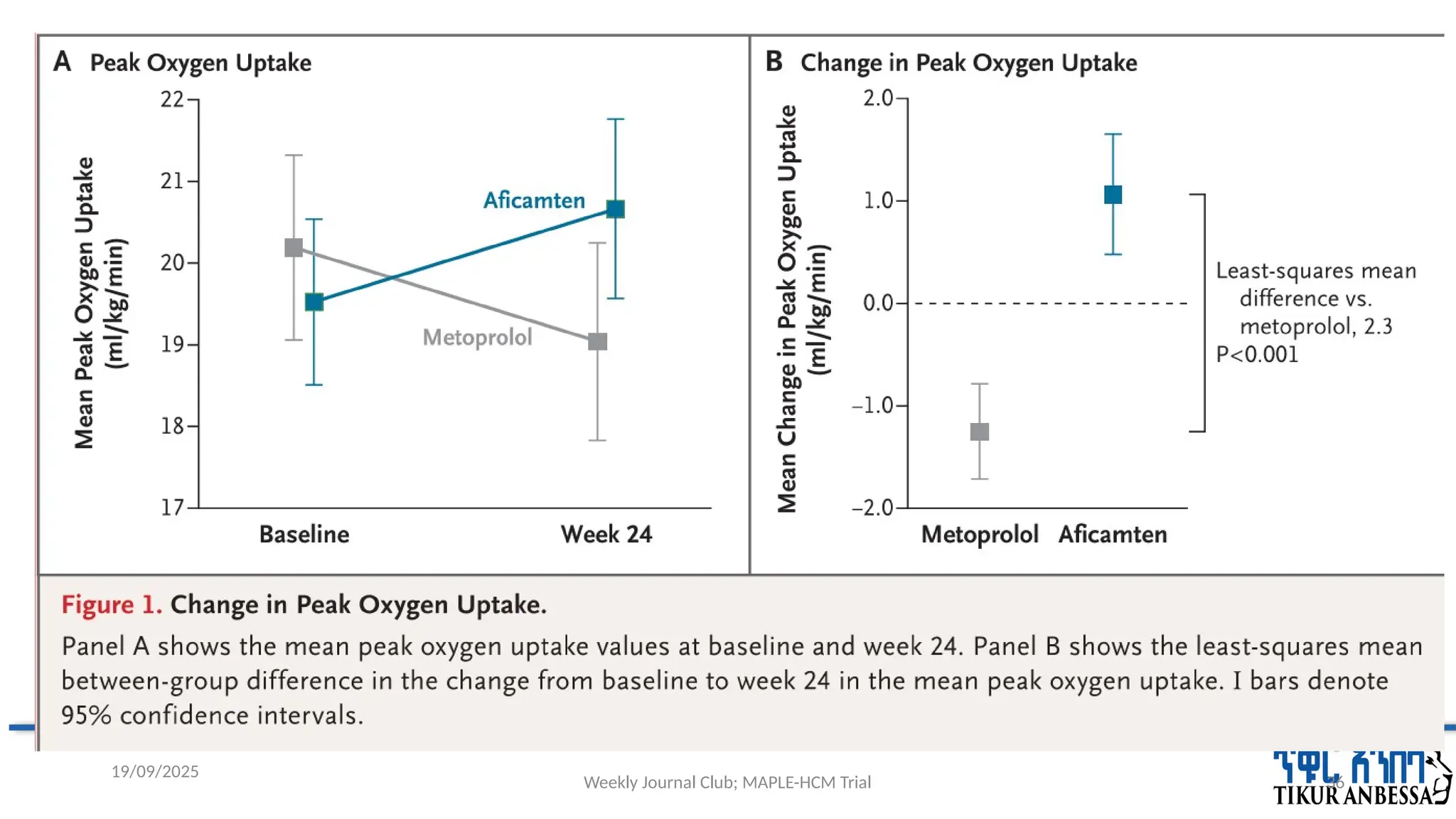
in patients with symptomatic oHCM, aficamten monotherapy was superior to metoprolol
monotherapy on the basis of improved peak oxygen uptake after a 24wk.
Aficamten treatment was also associated with decreased symptoms and improvements in LVOT
gradient, NT-proBNP level, and left atrial volume index.
The clinical benefits of aficamten as compared with metoprolol observed in this trial are probably
secondary to a decrease in LVOT obstruction resulting from CMI.
Parallel to the change in hemodynamics, aficamten reduced the NT-proBNP level, which is
predictive of future adverse outcomes related to HCM, including heart failure.
19/09/2025
46.
Weekly Journal Club;MAPLE-HCM Trial 46
cont'd...
The effect of aficamten on exercise capacity appeared to be consistent across all prespecified
subgroups
In addition to providing information on the use of aficamten as monotherapy (and as first-line
therapy in a subpopulation of patients with oHCM), this trial also provides unique insights into the
dose administration,
treatment effects, and
side effects of metoprolol in patients with oHCM.
19/09/2025
47.
Weekly Journal Club;MAPLE-HCM Trial 47
Strength
the first Phase 3 multicenter, double-blind, head-to-head comparison of aficamten to current
standard of care (metoprolol)in adults with symptomatic oHCM
first RCT to recommend aficamten as monotherapy for treatment of oHCM.
provides unique insights into the dose administration, treatment effects, and side effects of
metoprolol in patients with obstructive HCM.
trial met its primary and secondary endpoints
19/09/2025
48.
Weekly Journal Club;MAPLE-HCM Trial 48
Limitation
short treatment period,
the patients enrolled in this trial had objectively less-severe measures of disease burden
We cannot exclude the possibility that other non vasodilating beta-blockers have effects different
from those of metoprolol.
bias regarding investigator assumption of treatment assignment was possible given the negative
chronotropic effect of metoprolol.
blacks were under represented
19/09/2025
Weekly Journal Club;MAPLE-HCM Trial 50
Conclusion
this trial aimed at producing the necessary evidence to inform the use of
aficamten as potential first-line monotherapy, and its placement among the
pharmacologic option for oHCM.
19/09/2025
Weekly Journal ClubMAPLE-HCM-trial
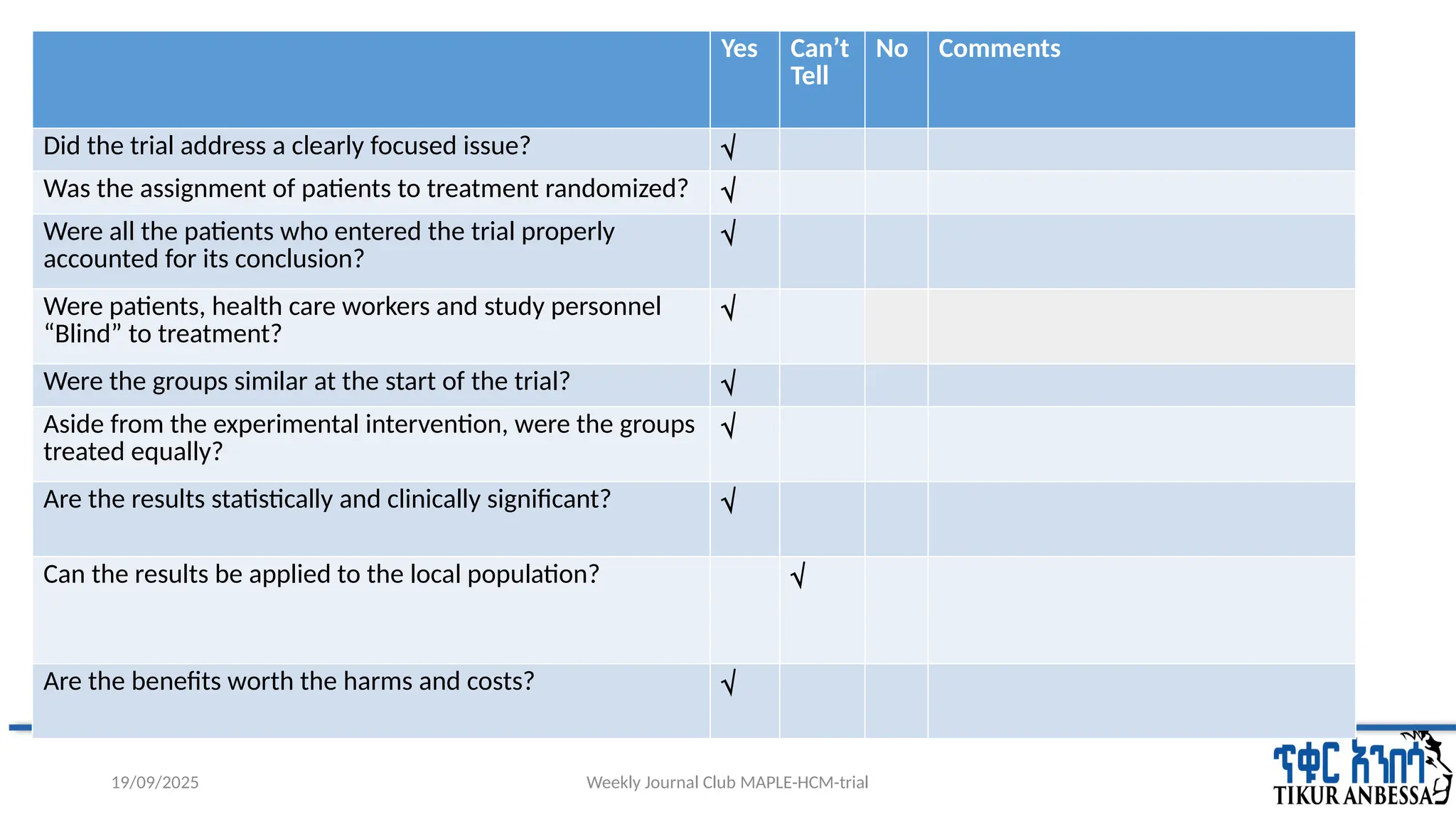
Critical Appraisal
19/09/2025
Yes Can’t
Tell
No Comments
Did the trial address a clearly focused issue? √
Was the assignment of patients to treatment randomized? √
Were all the patients who entered the trial properly
accounted for its conclusion?
√
Were patients, health care workers and study personnel
“Blind” to treatment?
√
Were the groups similar at the start of the trial? √
Aside from the experimental intervention, were the groups
treated equally?
√
Are the results statistically and clinically significant? √
Can the results be applied to the local population? √
Are the benefits worth the harms and costs? √
#1 Good morning every one and well come to today’s weekly journal club. My name is..., Internal medicine year 3 resident and I will be presenting MAPLE-HCM-trial, which was Published on AUGUST 30 2025
#2 The MAPLE-HCM (Metoprolol versus Aficamten in Patients with Left Ventricular Outflow Tract Obstruction on Exercise Capacity in HCM) trial
#3 Here is the outline that I will proceed throughout my presentation…
#10 • Although beta-blockers have been shown to reduce symptom burden and improve hemodynamics,
they do not improve exercise capacity and can be associated with poor tolerability.
Moreover, there are no controlled data on the long-term effects of beta-blockers on cardiac structure and function.
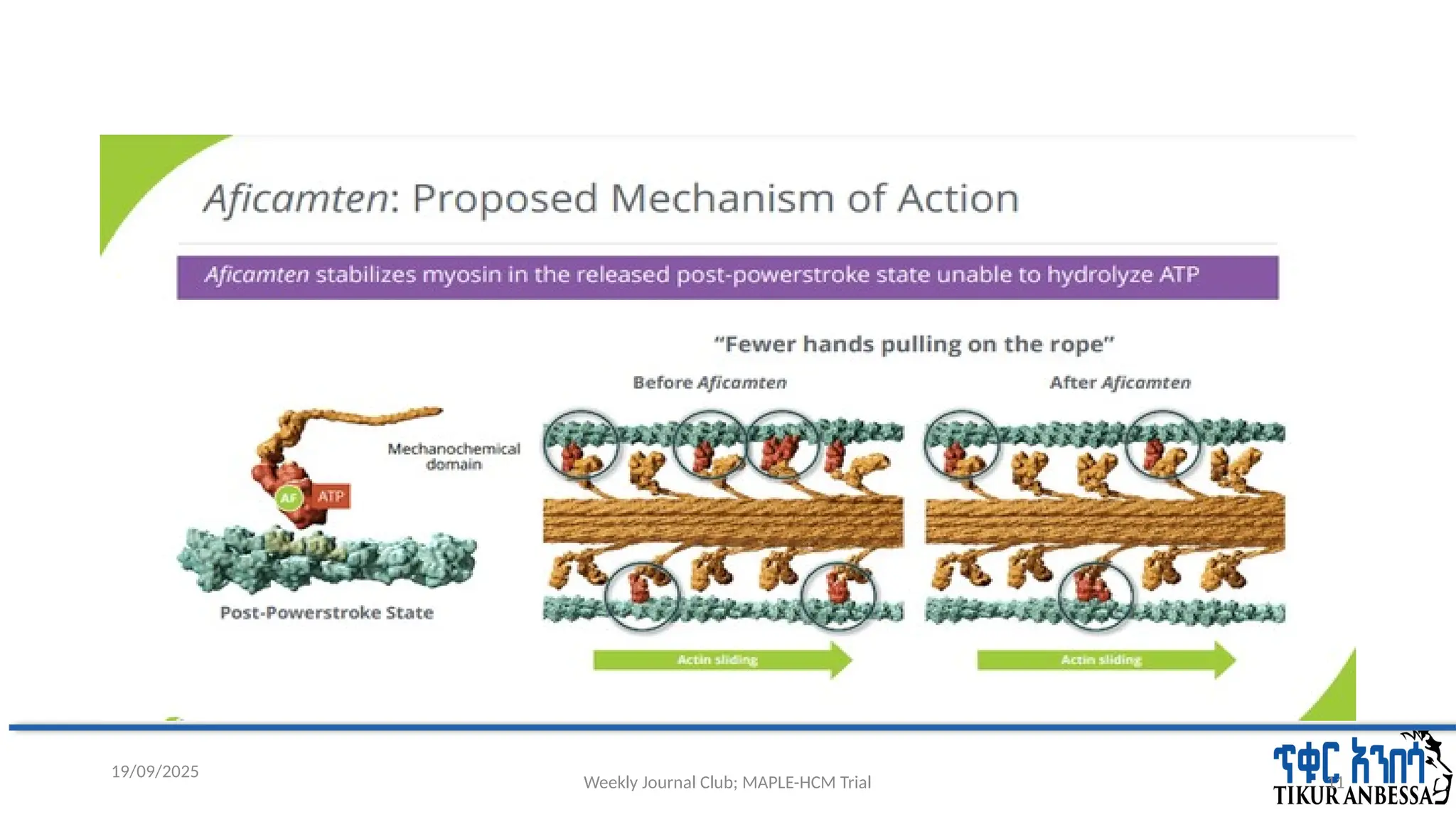
#11 • Aficamten is a next-in-class cardiac myosin inhibitor (CMI) that selectively and reversibly stabilizes the
lever arm of cardiac myosin in the relaxed position, decreasing the number of myosin molecules bound
to actin, resulting in decreased contractility .
Whether aficamten as monotherapy provides greater clinical benefit than beta-blockers as monotherapy remains unknown.
#12 Aficamten is a next-in-class cardiac myosin inhibitor that reduces myocardial hypercontractility by decreasing the number of active actin myosin cross-bridges within the sarcomere.
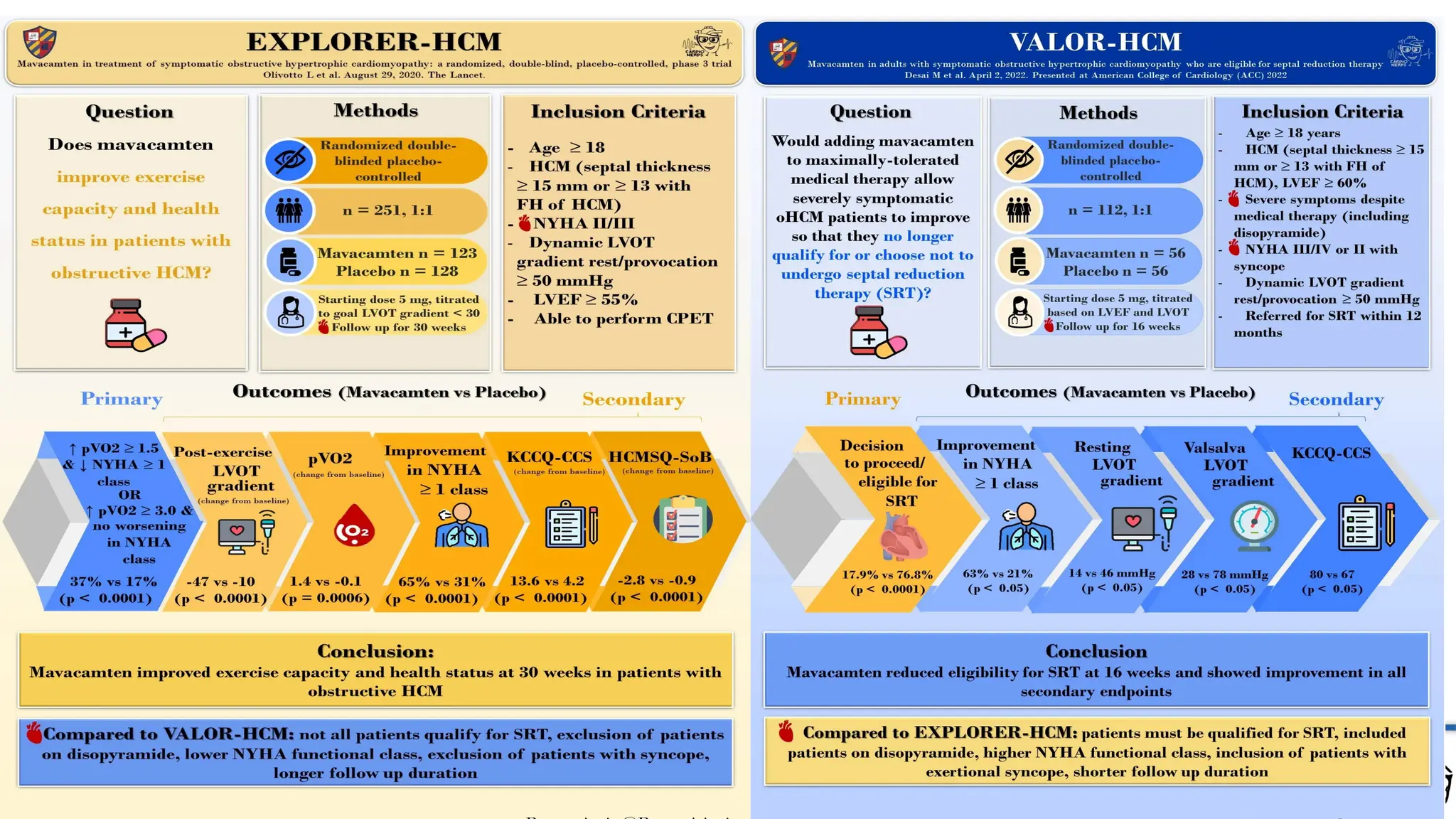
#15 HCMSQ-SoB => Hypertrophic Cardiomyopathy Symptom Questionnaire – Shortness of Breath domain.
The Phase 2 REDWOOD-HCM study demonstrates that treatment with aficamten for 10 weeks was generally well tolerated in participants with symptomatic oHCM.There were also marked improvements in LVOT-G (resting and Valsalva), NYHA functional class(FC), and cardiac biomarkers (NT-proBNP and hs-cTnI).
#17 The MAPLE-HCM (Metoprolol versus Aficamten in Patients with Left Ventricular Outflow Tract Obstruction on Exercise Capacity in HCM) trial .
=>Whether aficamten as monotherapy provides greater clinical benefit than beta-blockers as monotherapy remains unknown.
#18 The MAPLE-HCM (Metoprolol versus Aficamten in Patients with Left Ventricular Outflow Tract Obstruction on Exercise Capacity in HCM) trial
#21 . Only an independent data monitoring committee had access to and reviewed unblinded safety data during the conduct of the trial.
.... performed by Fortrea, a contract research organization.
#22 Approximately 10% of oHCM patients who were previously treated with mavacamten can participate in the study with Medical
Monitor approval.
#24 Patients underwent randomization within 6 weeks after the start of screening. If applicable,patients underwent a washout of background standard therapy of up to 2 weeks beginning at the first screening visit. At the discretion of the investigator, patients reduced the dose of standard medications every 2 days until standard medications were discontinued for at least 7 days before screening assessments.
#26 Treatment was followed by a 4-week washout period, during which patients discontinued aficamten and its matching placebo or were weaned off metoprolol and its matching placebo during the initial 2 weeks.
Patients were followed from the time of randomization to their final visit, irrespective of whether they continued to receive the trial drug.
#27 The primary analysis tested the null hypothesis that there would be no between-group difference in peak oxygen uptake in the full analysis population.
#30 Patients assigned to receive aficamten started at a dose of 5 mg once daily and escalate to doses of 10, 15, and 20 mg once daily if they meet the 2 echocardiographic escalation criteria (LVEF ≥55% and post-Valsalva LVOT gradient ≥30 mm Hg) or remain at their current doses if escalation criteria are not met. Patients assigned to metoprolol start at a dose of 50 mg once daily and escalate to doses of 100, 150, and 200 mg once daily if they meet the 2 echocardiographic (LVEF ≥55% and post-Valsalva LVOT gradient ≥30 mm Hg) and 2 vital sign criteria (systolic blood pressure ≥90 mm Hg and heart rate ≥55 beats/min) or remain at their current doses if any of the escalation criteria are not met.
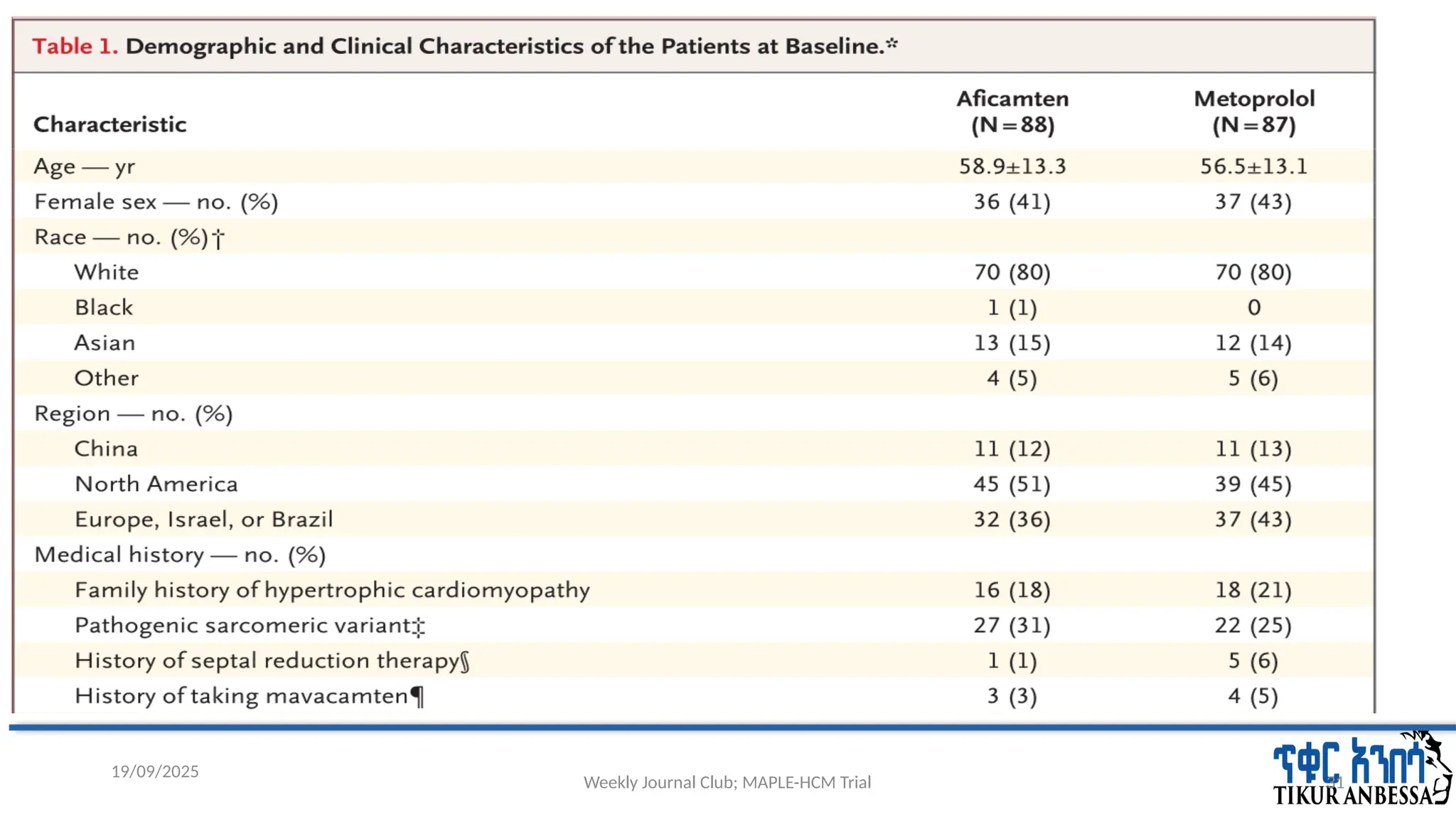
#31 † Race was reported by the patients. “Other” includes other, not reported, and not known.
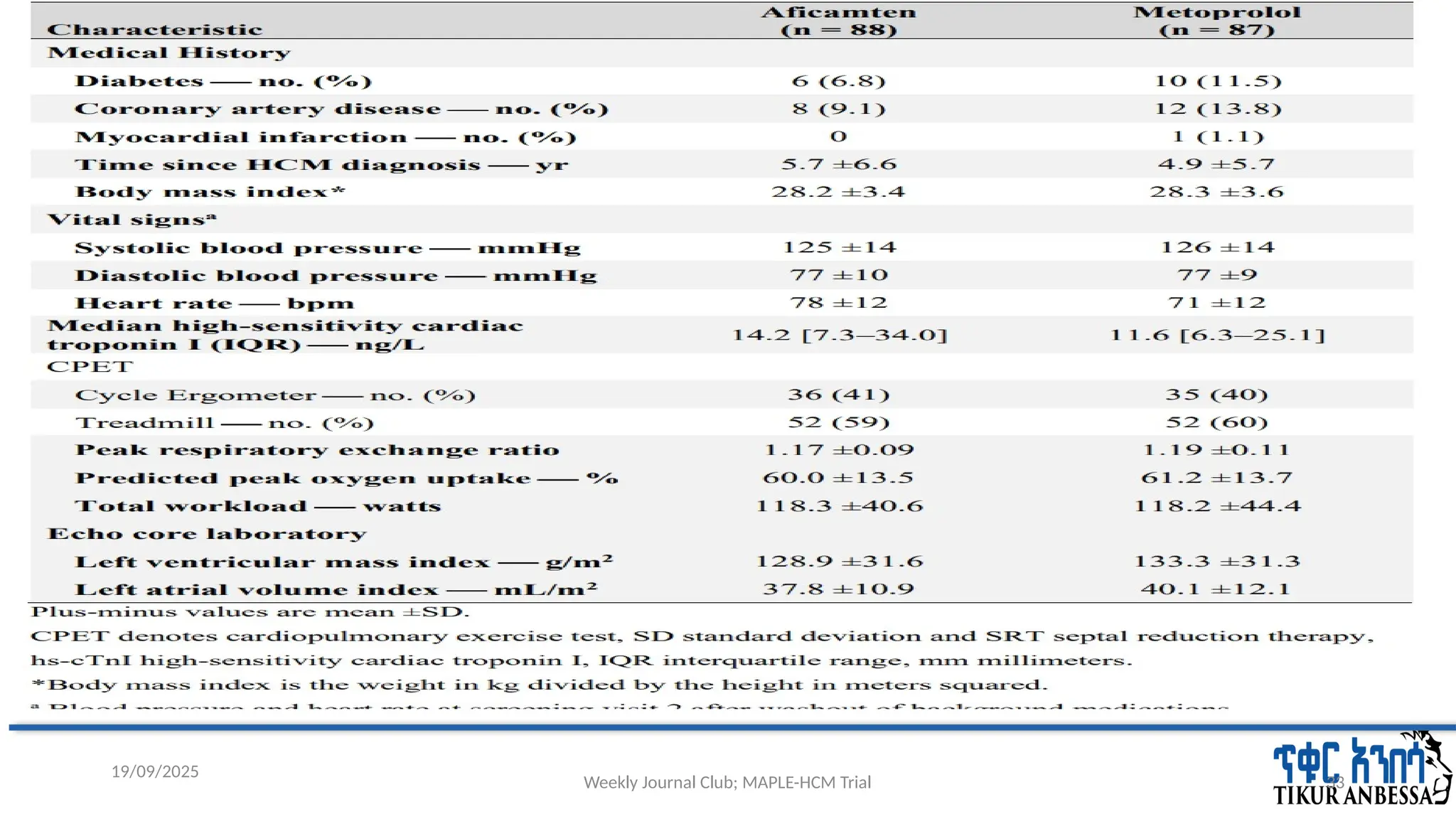
#32 * Plus–minus values are means ±SD. Percentages may not total 100 because of rounding. IQR denotes interquartile range, and NT-proBNP N-terminal pro–B-type natriuretic peptide.
† Race was reported by the patients. “Other” includes other, not reported, and not known.
‡ Genetic testing required separate consent and was not performed in 37 patients (18 in the aficamten group and 19 in the metoprolol group).
§ Patients who had not yet undergone screening and remained symptomatic more than 6 months after septal reduction therapy were included. Of the six patients with a history of septal reduction therapy, two had a history of alcohol septal ablation (both in the metoprolol group) and four had a history of myectomy (one in the aficamten group and three in the metoprolol group).
¶ Patients previously exposed to mavacamten were allowed to participate if they had not received mavacamten for at least 8 weeks before screening and had no safety issues.
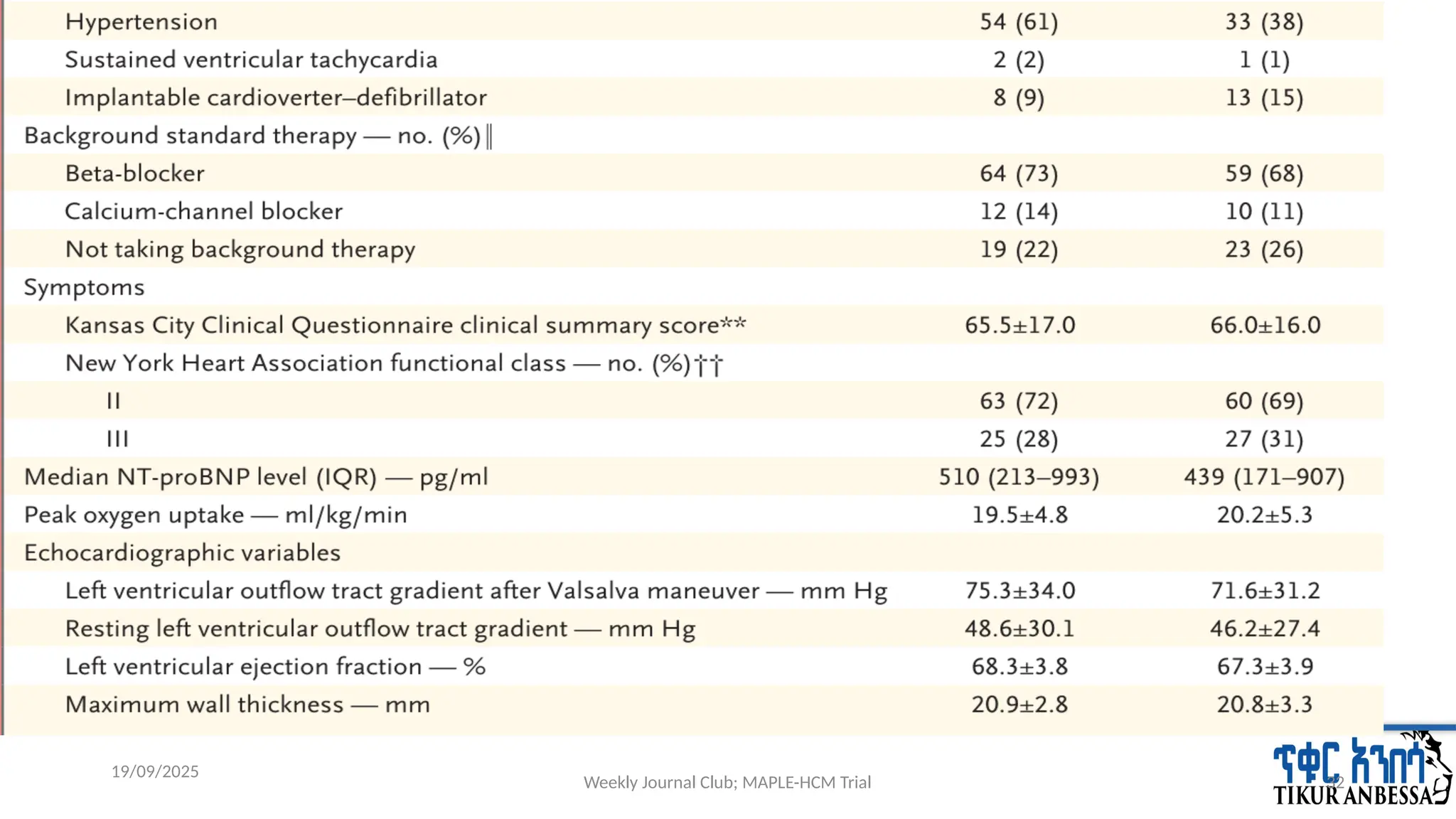
‖ Background standard therapy included medications taken at the time of initial screening, before screening washout.
** Scores range from 0 to 100, with higher scores indicating fewer symptoms and physical limitations.
†† Functional classes range from I to IV, with higher values indicating greater disability.
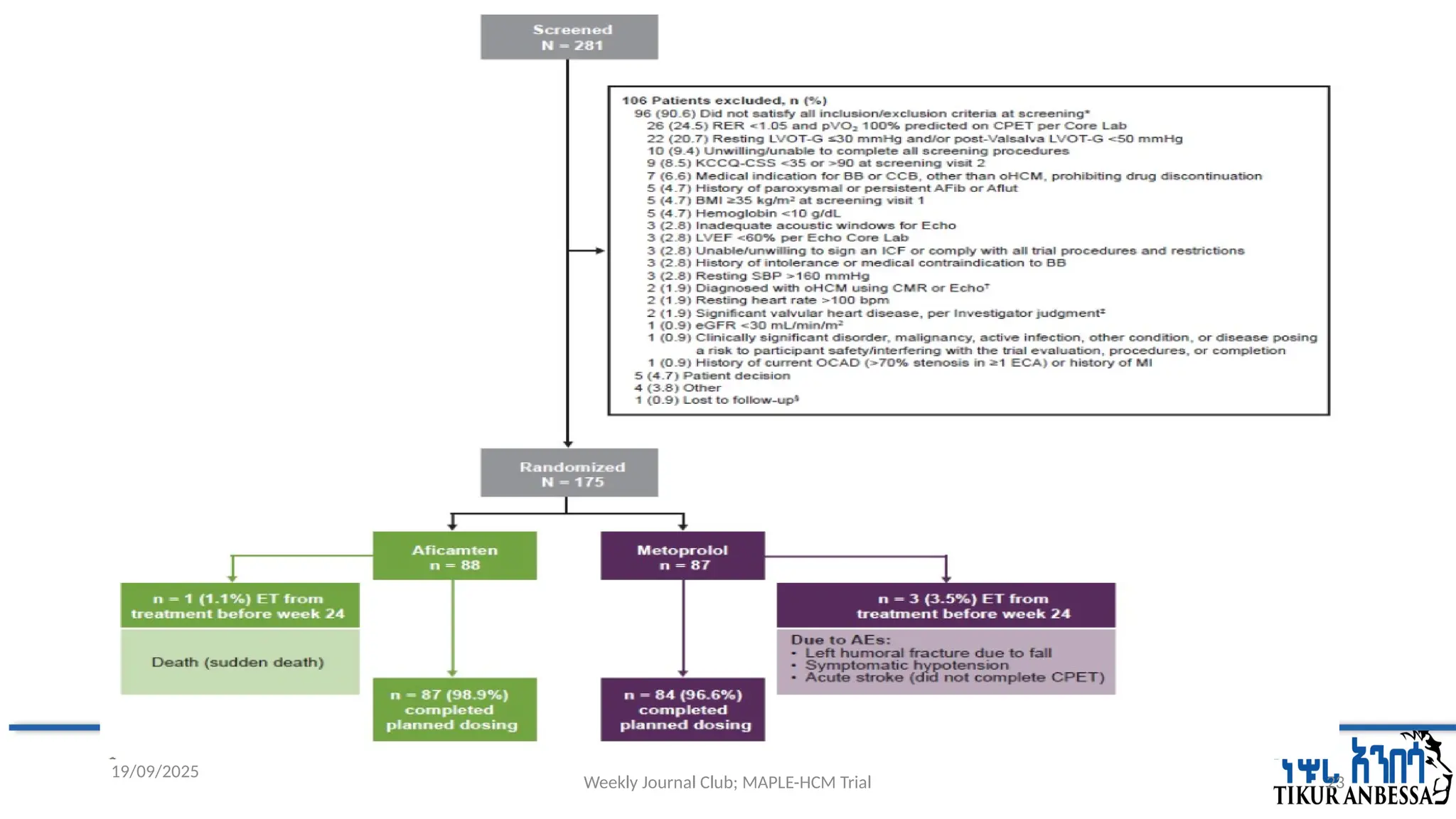
#34 From June 20, 2023, to August 9, 2024, a total of 281 patients were screened for eligibility at 71 sites in North America, Brazil, Europe, Israel, and China; 175 patients underwent randomization.
A total of 88 patients were randomly assigned to the aficamten group and 87 to the metoprolol group.
Of these patients, 171 completed the trial treatment;
3 patients assigned to the metoprolol group discontinued treatment because of adverse events but completed trial visits, and 1 patient assigned to the aficamten group died before the end of the trial
The mean age of the patients was 58 years, and 58.3% were men.
At baseline,
the mean LOVT gradient at rest was 47 mm Hg and after the Valsalva maneuver was 74 mm Hg,
the mean LVEF was 68%, and
70.3% of patients had NYHA class II heart failure.
Overall, 53 patients (30.3%) had a new HCM diagnosis or had not previously received treatment.
At the end of the dose-adjustment period (week 8):
among the patients assigned to receive aficamten,
67 (77%) were receiving high dose (15mg or 20mg) of aficamten
Among the patients assigned to receive metoprolol,
55 (64%) were receiving 150mg or 200mg of metoprolol
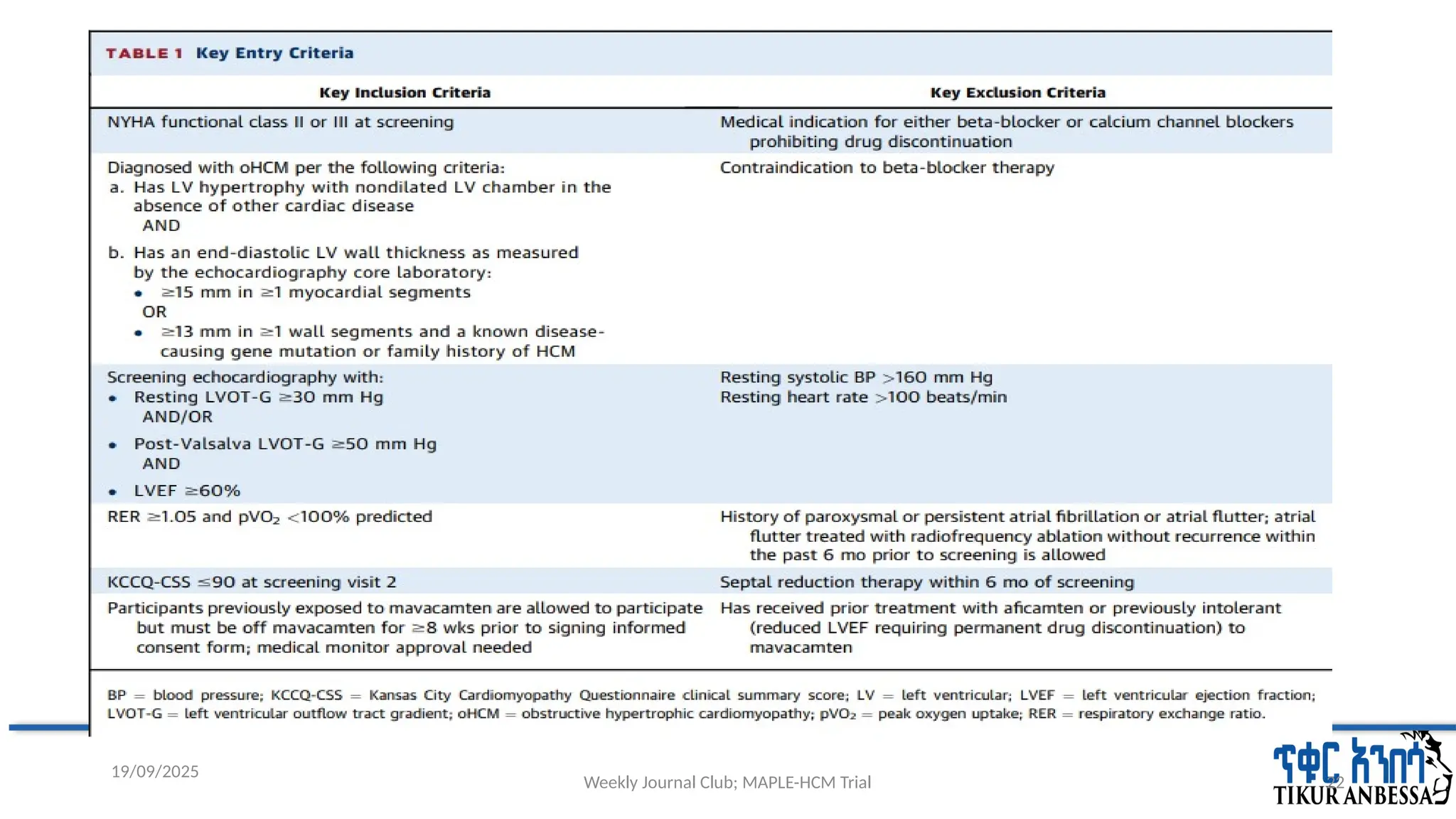
The most common reasons for exclusion from trial participation were below-threshold left ventricular outflow tract gradients and not meeting cardiopulmonary exercise testing criteria.
#35 aficamten = 35 (40%) were receiving 15 mg, and 31 (36%) were receiving 20 mg,
metoprolol= 19 (23%) were receiving 150 mg, and 34 (40%) were receiving 200 mg,
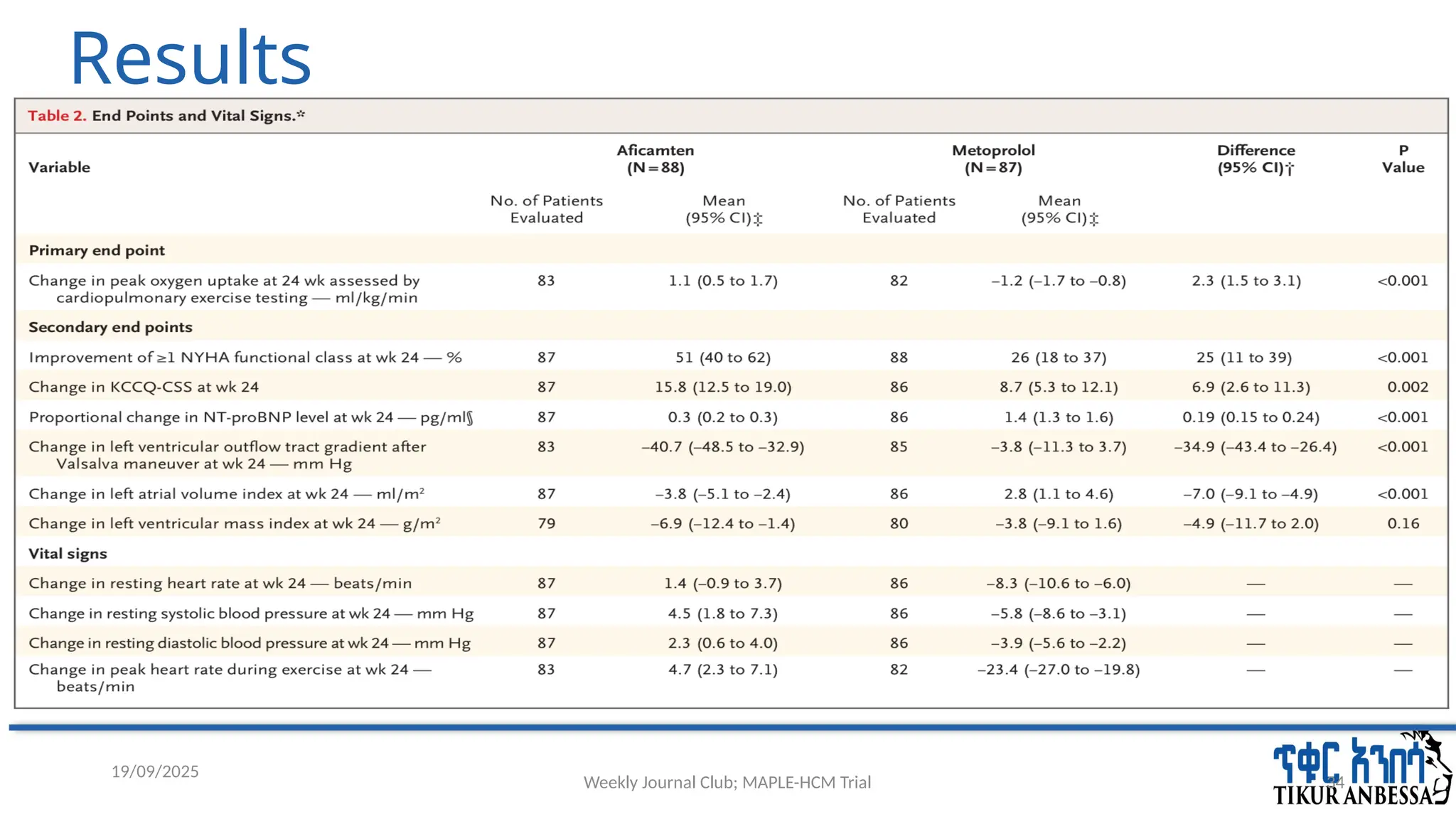
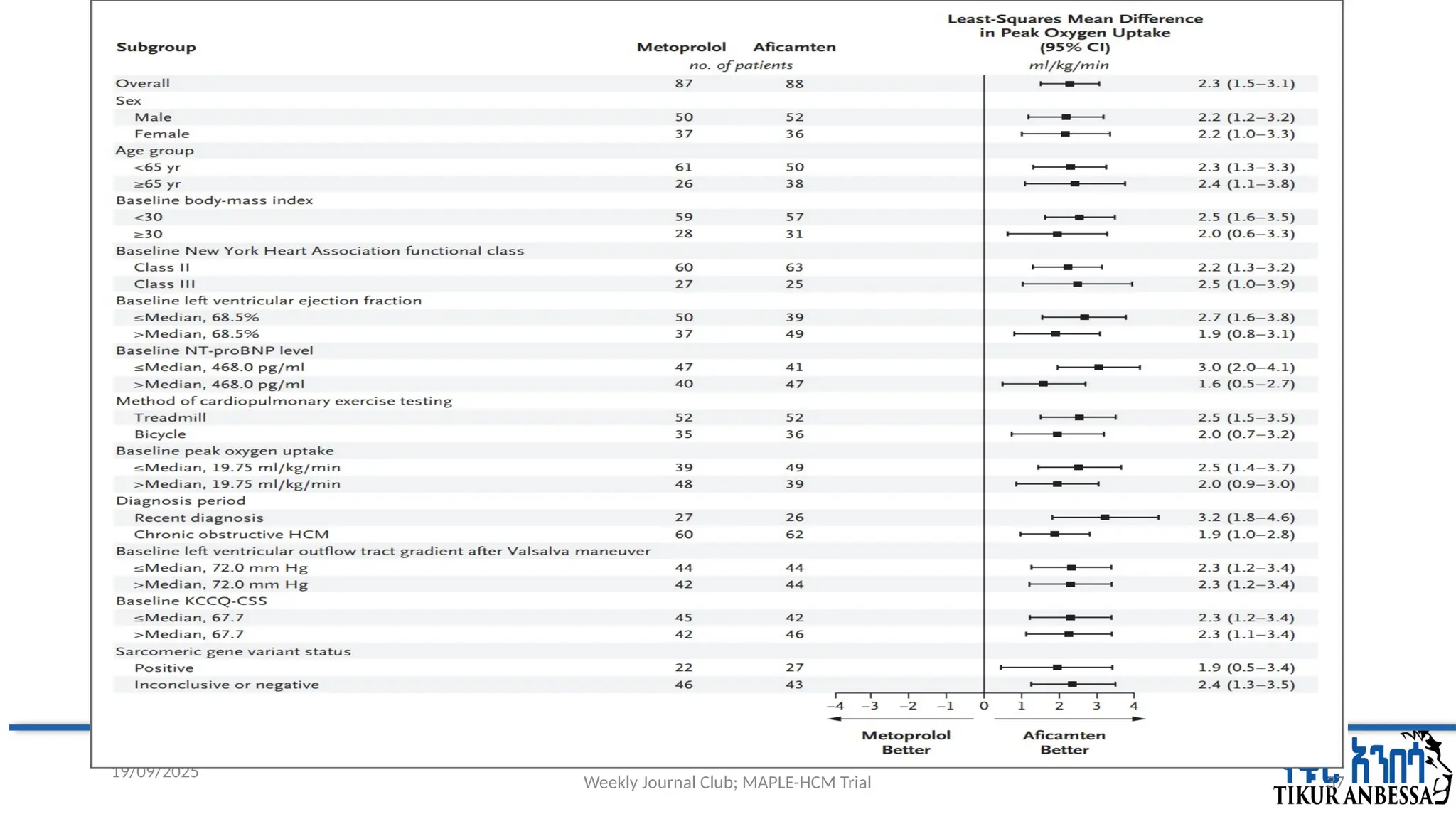
#37 The treatment effect appeared to be consistent across all prespecified subgroups (Fig. 2).
The mean change from baseline to week 24 in peak heart rate during cardiopulmonary exercise testing was 4.7 beats per minute (95% CI, 2.3 to 7.1) in the aficamten group and −23.4 beats per minute (95% CI, −27.0 to −19.8) in the metoprolol group.
Values for peak oxygen uptake at week 24 were missing or invalid for 10 patients (5.7%; 5 in each group).
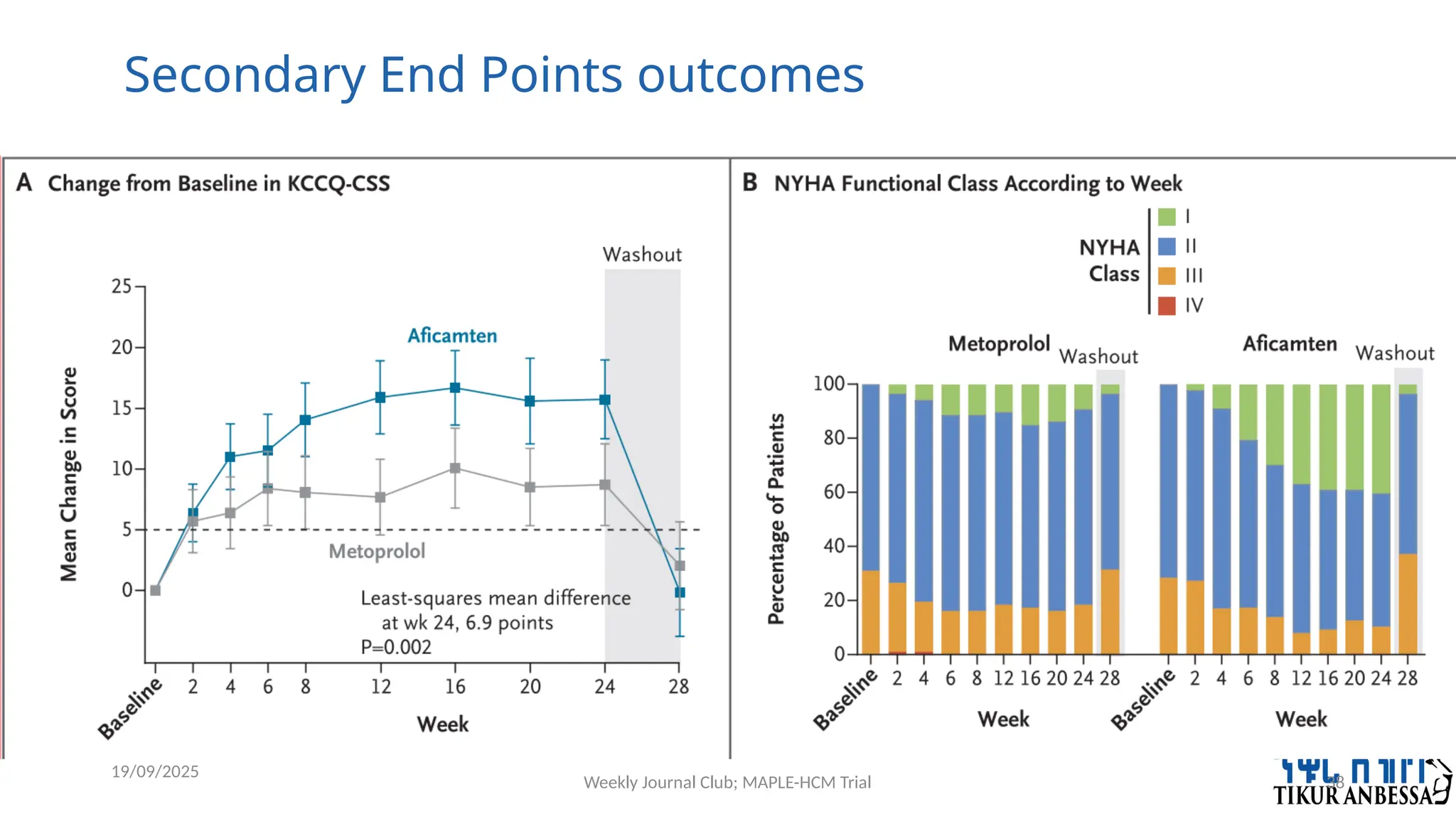
#38 Key Secondary End Points.Panel A shows the change from baseline in the KCCQ-CSS. The dashed line indicates the minimum clinically important difference. Panel B shows the percentage of patients in each New York Heart Association (NYHA) functional class at baseline and at 2-week or 4-week increments
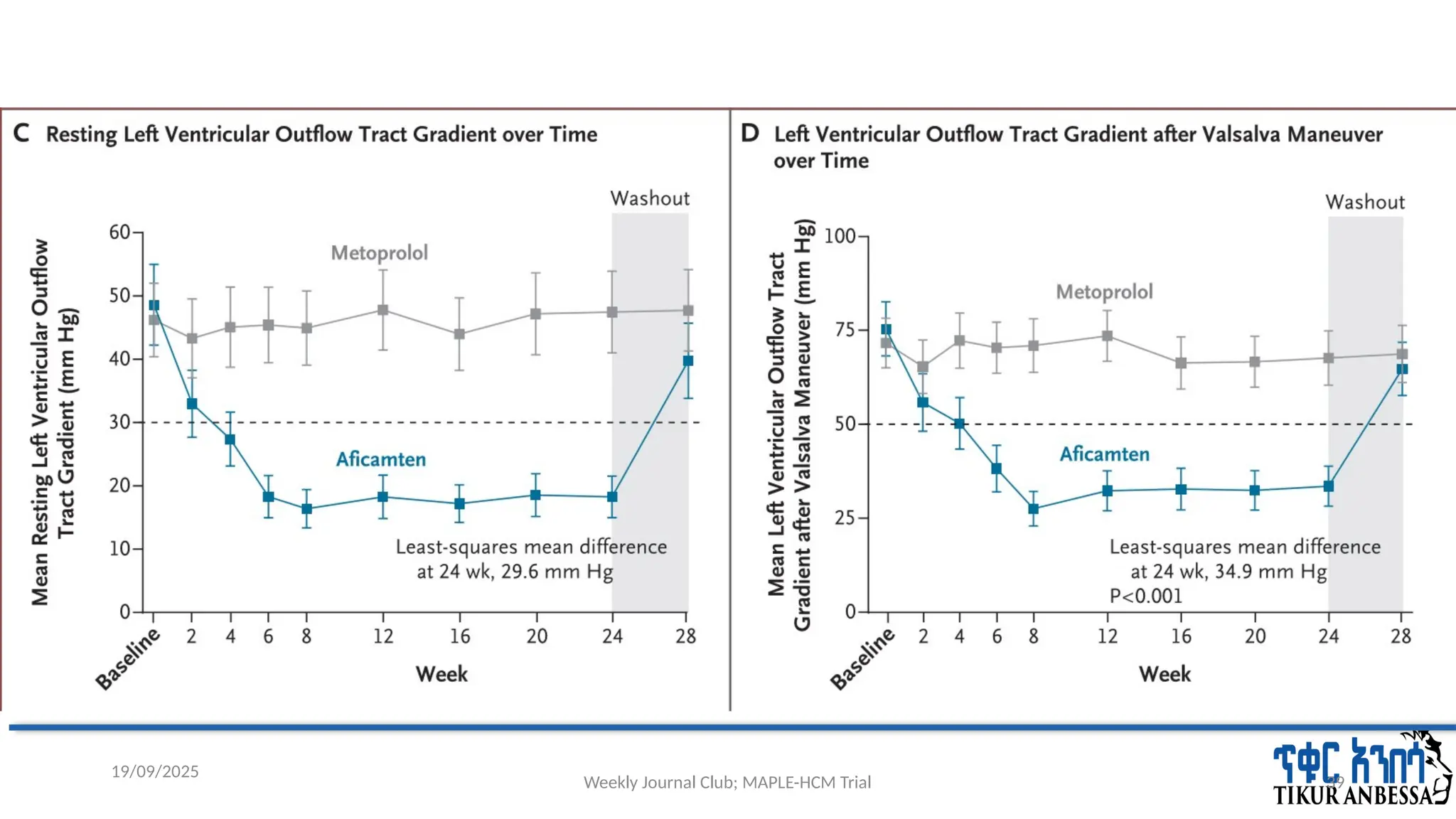
#39 Panel C shows the mean resting left ventricular outflow tract gradient over time (exploratory end point). Panel D shows the mean left ventricular out flow tract gradient after the Valsalva maneuver over time. The dashed lines in Panels C and D denote the minimum value indicative of obstructive HCM.
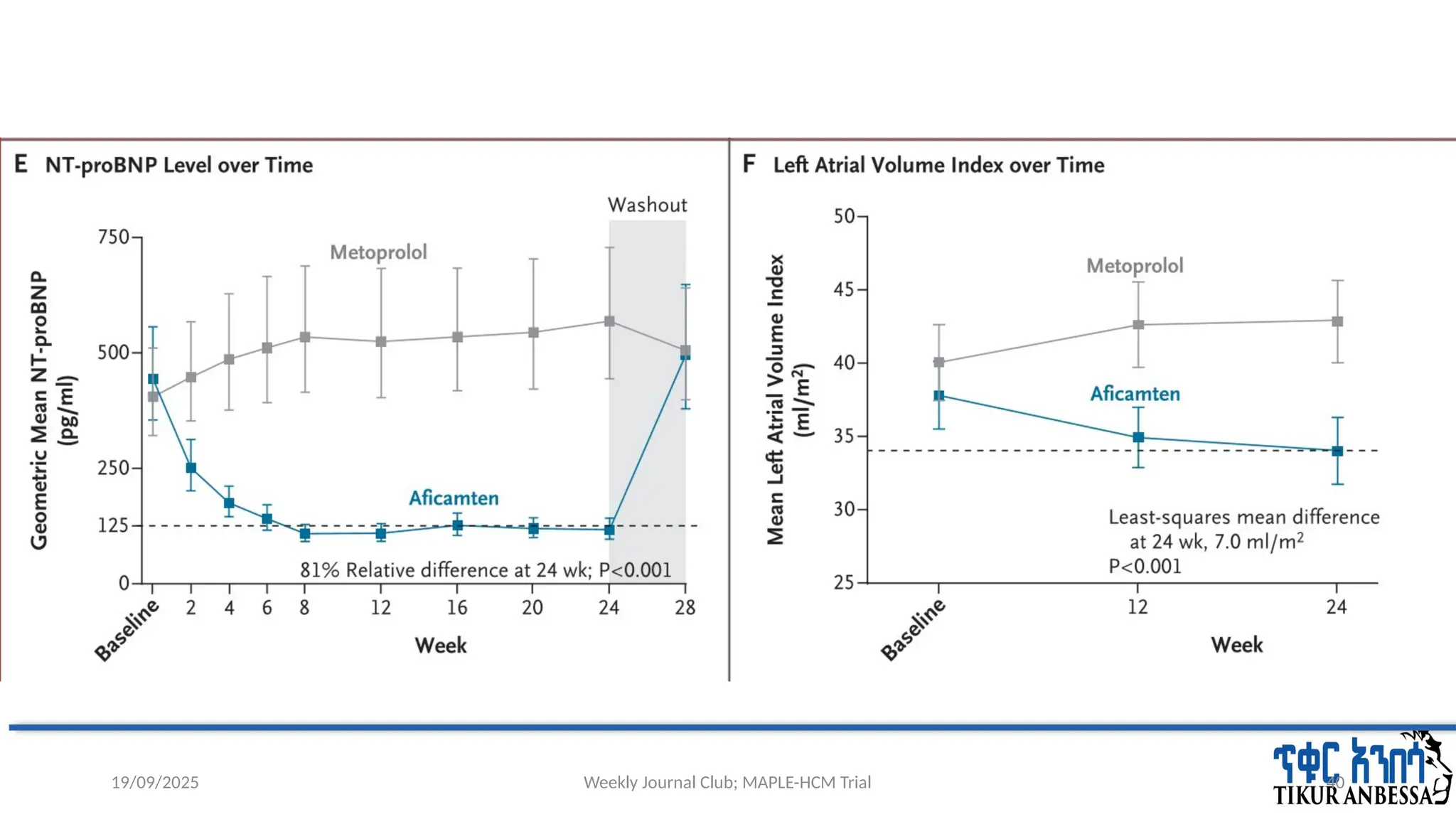
#40 Panel E shows the geometric mean NT-proBNP level over time. Panel F shows the mean left atrial volume index over time. The dashed lines in Panels E and F indicate the upper limit of the normal range. All echocardiographic and biomarker values shown are based on core laboratory measurements. I bars denote 95% confidence intervals.
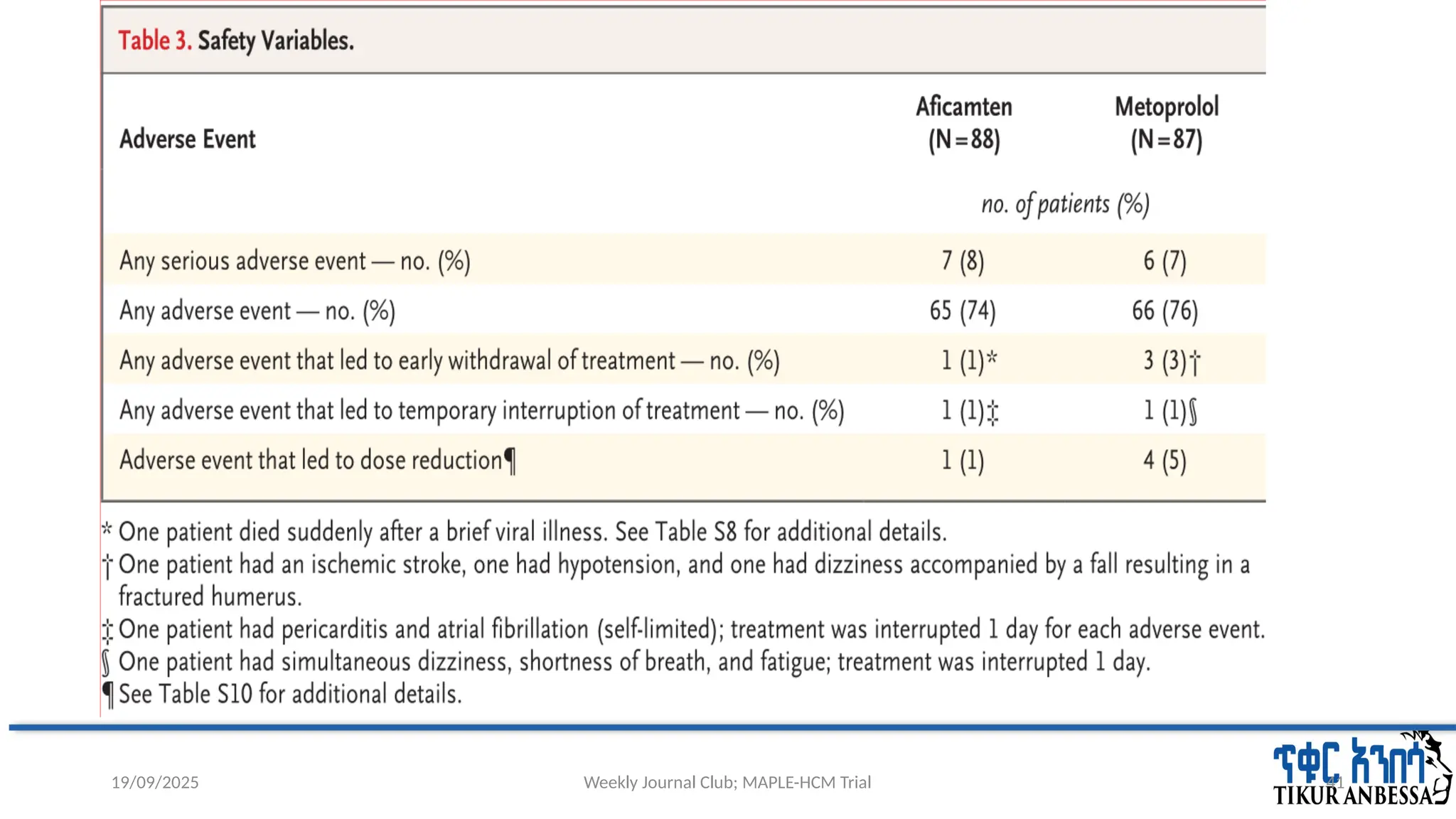
#41 death=a 69-year-old female with history of oHCM, Type 2 diabetes mellitus, hypertension, hypercholesterolemia, breast cancer (stage 1), left bundle branch block, mild mitral valve stenosis, no implantable cardioverter defibrillator or major HCM-specific sudden cardiac death risk factors. At Week 4, the echo showed LVEF 60% (~6% decreased from baseline) with LVOT gradients similar to baseline; NT-proBNP and hs-cTnI were decreased compared to baseline by 44% and 54%, respectively; KCCQ CSS was increased by 6 points; she was uptitrated to 15 mg aficamten per protocol. Before the Week 6 visit, the patient reported upper respiratory infection symptoms. She experienced unwitnessed sudden death. No autopsy was performed. There was no evidence of systolic dysfunction, or signs or symptoms of heart failure prior to her sudden death. Plasma concentrations of aficamten increased appropriately
with up-titration.
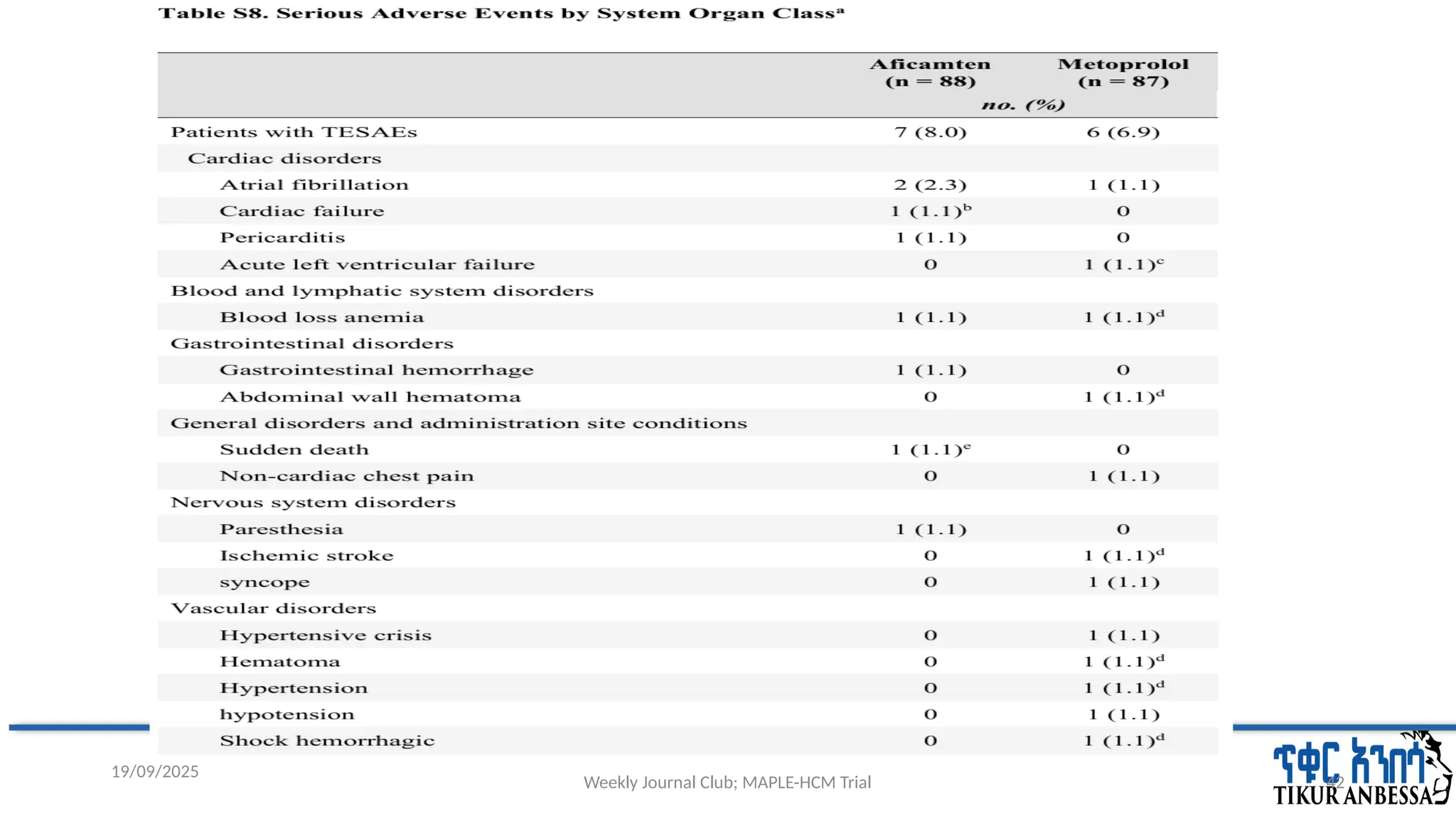
#42 a=Number (%) of participants with TESAEs, sorted by descending frequency.
b=Occurred after end of treatment
c=Acute on chronic diastolic congestive heart failure; no decrease in LVEF
d=Same patient.
#44 a=Three patients had four down-titration events per site-read LVEF <50% and one patient had a down titration due to an AE of dizziness.
b=26 patients had 31 down titration events including five patients who had two down-titration events each.
c=The four AEs leading to down titration among the metoprolol-treated patients were: light headedness (n = 2), low heart rate (n = 1), and fatigue (n = 1).
#45 Parallel to the change in hemodynamics, aficamten reduced the NT-proBNP level, which is predictive of future adverse outcomes related to HCM, including heart failure.
The effect of aficamten on exercise capacity appeared to be consistent across all prespecified subgroups, including among patients with a new diagnosis or who had
#48 which precludes assessment of the relative effect of aficamten and metoprolol on longer-term clinical outcomes.
the metoprolol dose-adjustment protocol used in this trial may differ from strategies used in local practice.