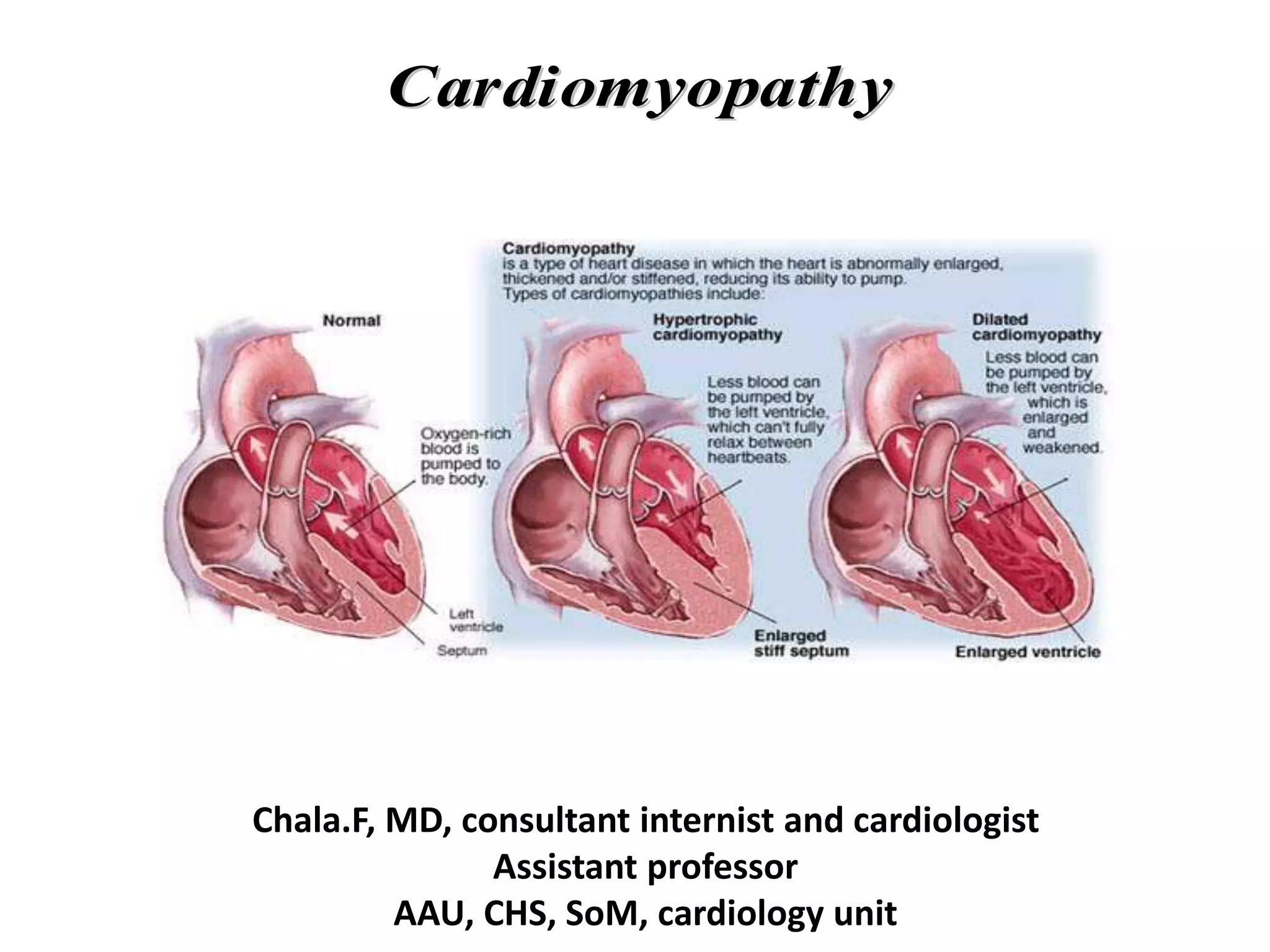
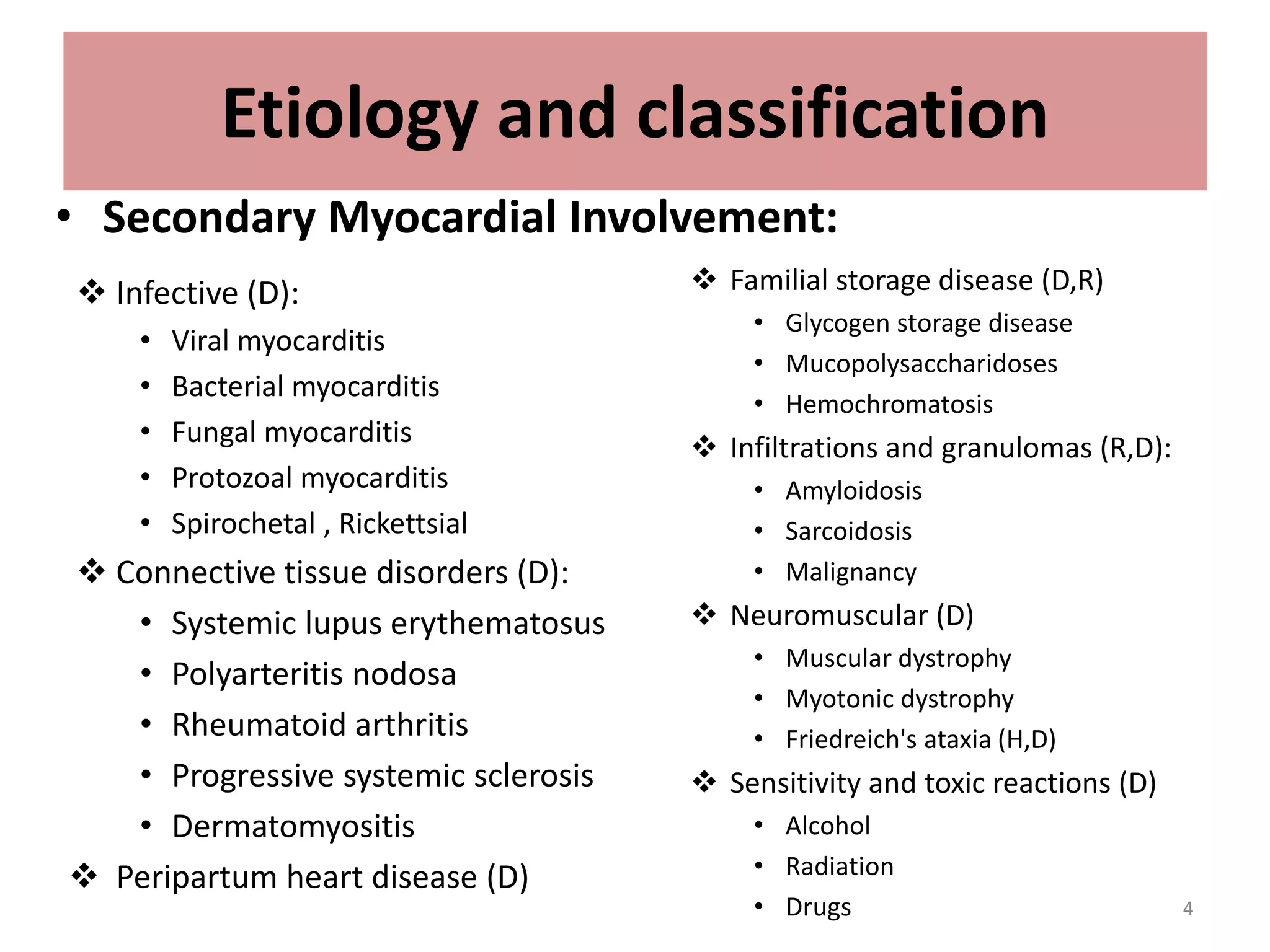
Cardiomyopathies are diseases of the heart muscle that are not caused by hypertension, coronary artery disease, valvular or pericardial abnormalities. They can be classified as primary (involving the myocardium of unknown cause) or secondary (caused by a systemic disease).
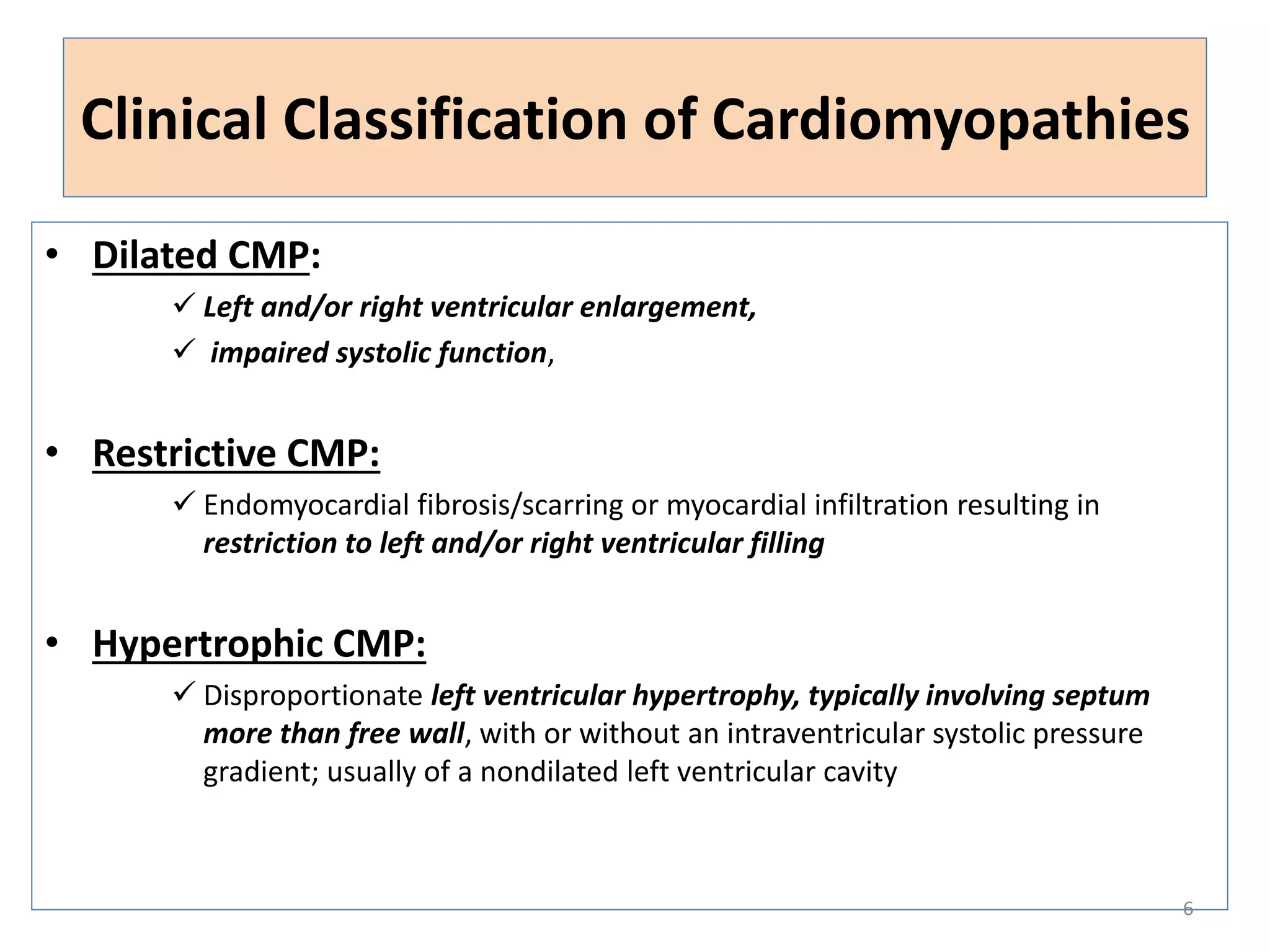
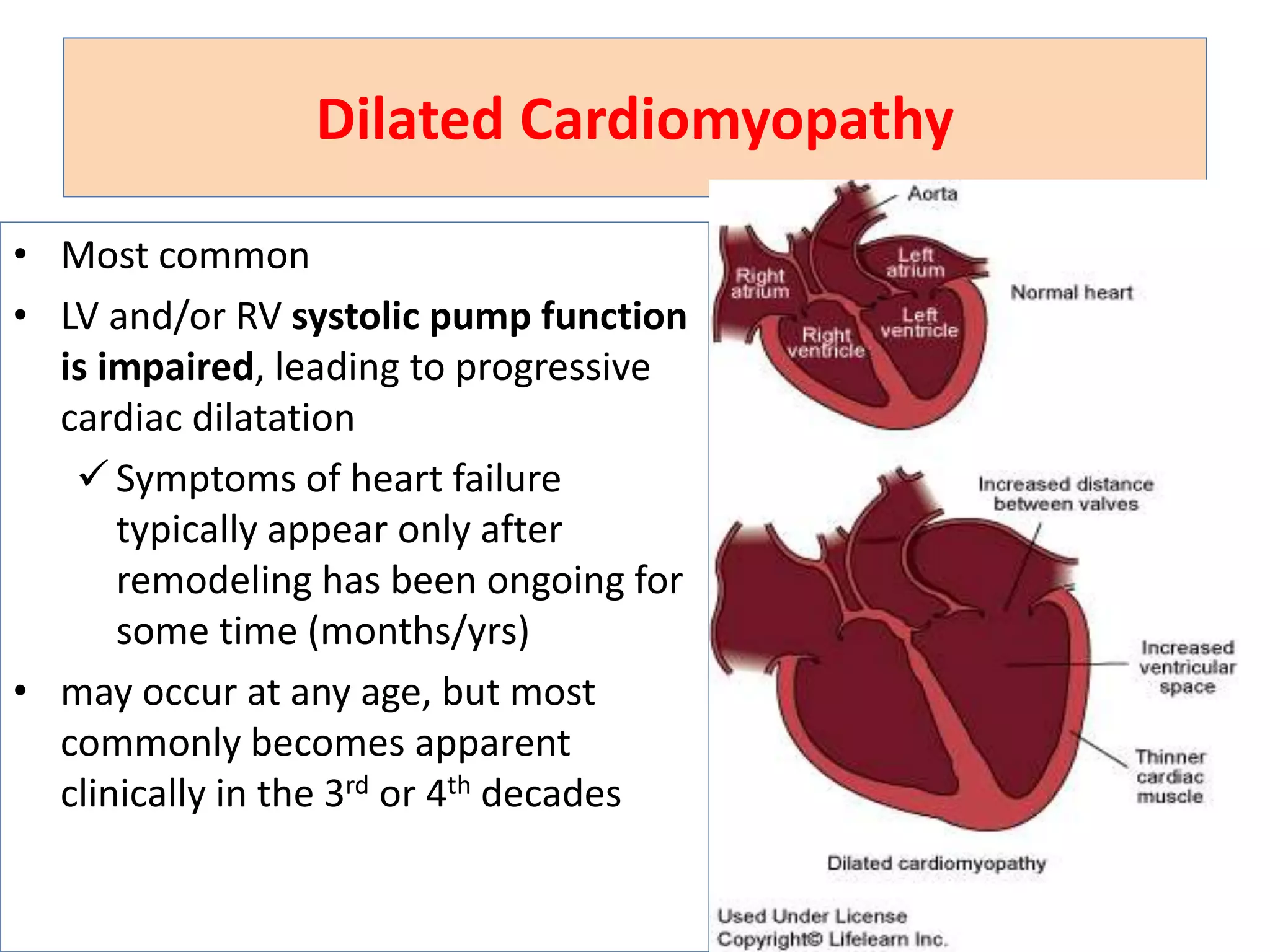
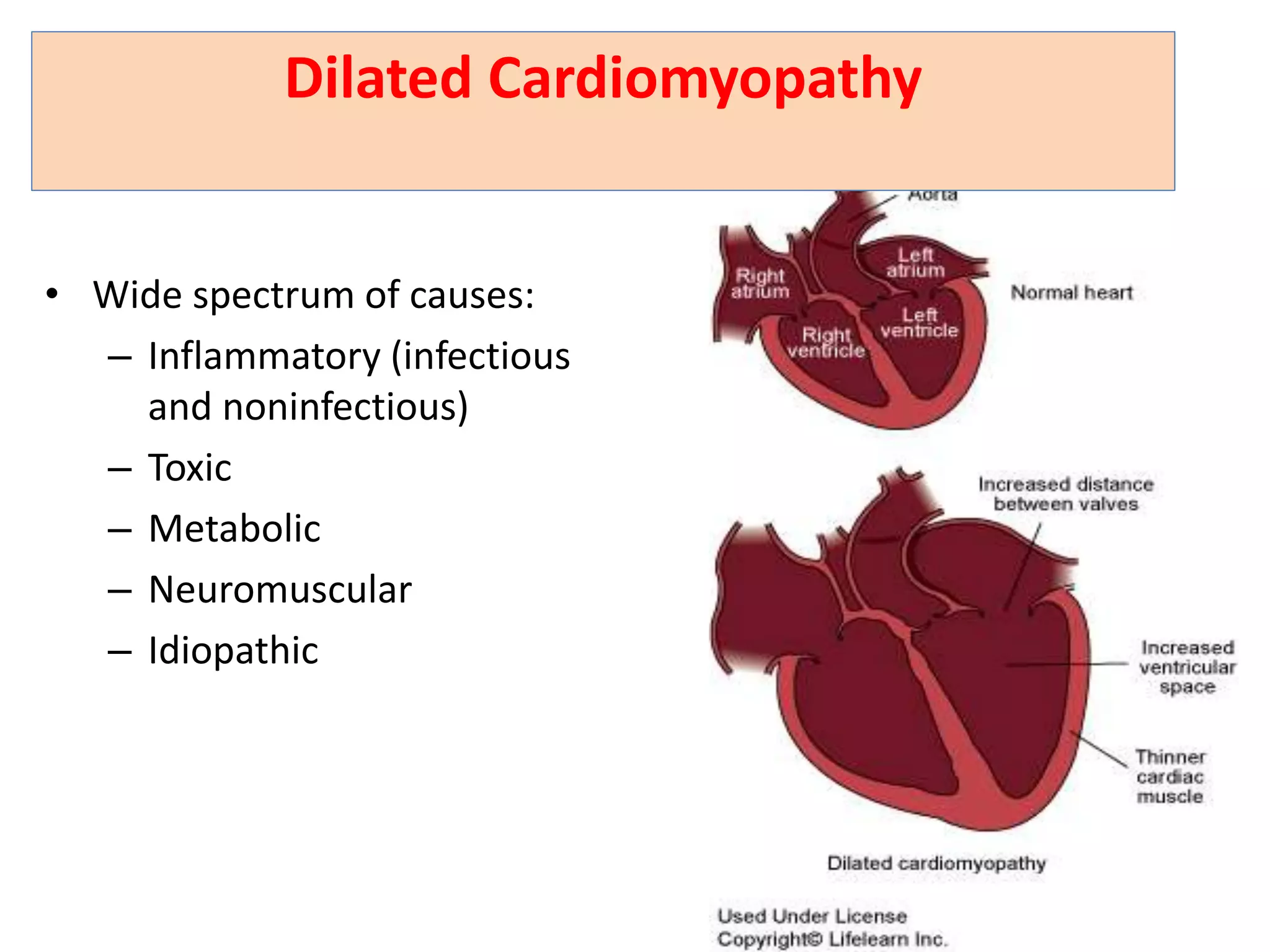
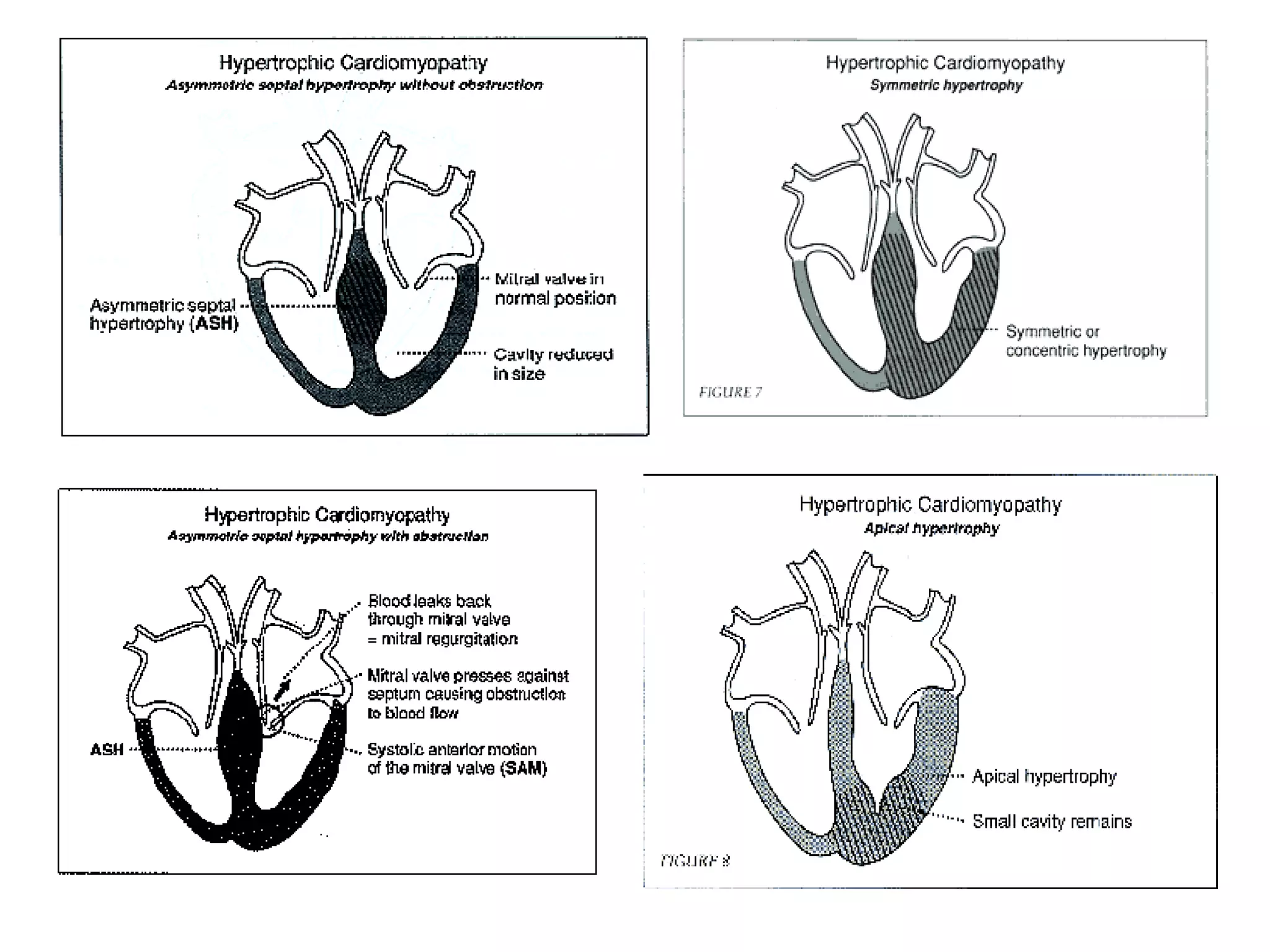
The document discusses the main types of cardiomyopathy - dilated, hypertrophic and restrictive. It provides details on their definitions, causes, clinical features, diagnostic evaluations and treatments. Dilated cardiomyopathy is the most common and causes ventricular enlargement and impaired systolic function. Hypertrophic cardiomyopathy causes disproportionate left ventricular hypertrophy. Restrictive cardiomyopathy results in stiff ventricles that impede filling.