P R ES E N T E D B Y : D R . A B E L W ( R 2 )
M O D E R A T O R : D R . S H A M I L
HAWASSA
COMPRENSIVE
SPECIALIZED COLLAGE
SEMINAR PRESENTATION ON THE PEARLS
OF PNEUMONIA
2.
2
Learning Objectives
• Recognizethe epidemiology and morbidity of pneumonia
• Define pneumonia and types of lower respiratory tract infections
• Understand features involved in the pathophysiology of
pneumonia
• Recognize the entity known as Community Acquired Pneumonia
(CAP)
• Appreciate the spectrum of pneumonia clinical presentation
• Identify common complications of pneumonia
3.
3
Pneumonia is commonand serious
• 5.6 million cases in US in 2011(1)
• 2nd
leading cause of hospitalization in US (1.1 million admissions in US)(1)
~20% of patients with pneumonia require hospitalization
• 6th
leading cause of death in US in 2011 (~60,000 deaths)(1)
~10% of patients with pneumonia die
Variations in rates of disease:
Anevlavis S; Bouros D (2010). Expert Opin Pharmacother 11 (3): 361–74.
• More common in children and
older adults
(overall rate for 18-49 yo is ~5 per
1000
overall rate for >65 yo is 75 per
1000 )
• Higher rates in winter months
• More common in men
• More common in African
Americans compared to
Caucasians
4.
4
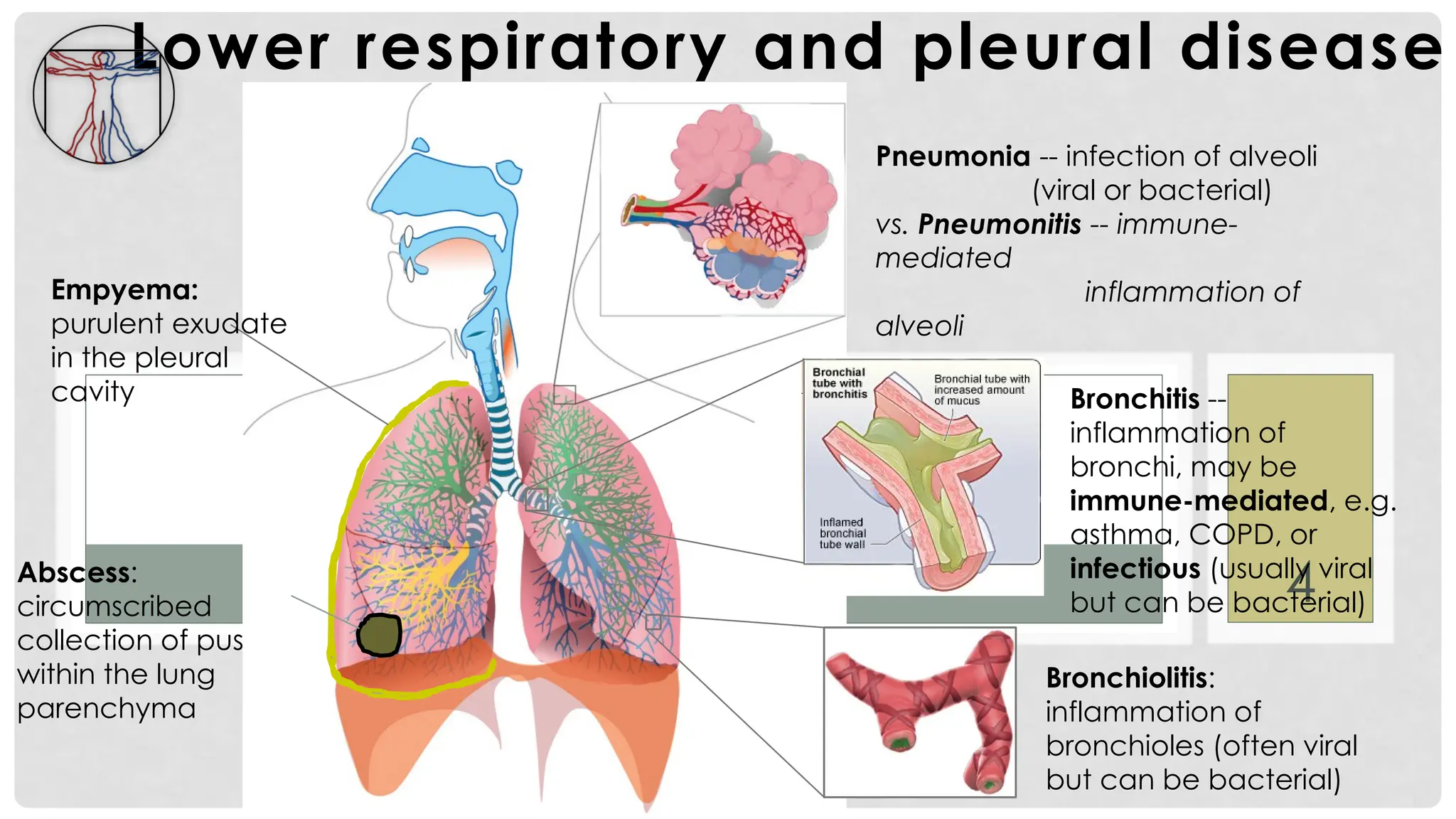
Lower respiratory andpleural disease
Pneumonia -- infection of alveoli
(viral or bacterial)
vs. Pneumonitis -- immune-
mediated
inflammation of
alveoli
Bronchitis --
inflammation of
bronchi, may be
immune-mediated, e.g.
asthma, COPD, or
infectious (usually viral
but can be bacterial)
Empyema:
purulent exudate
in the pleural
cavity
Abscess:
circumscribed
collection of pus
within the lung
parenchyma
Bronchiolitis:
inflammation of
bronchioles (often viral
but can be bacterial)
5.
5
PNEUMONIA:
CLEARANCE vs. COLONIZATION
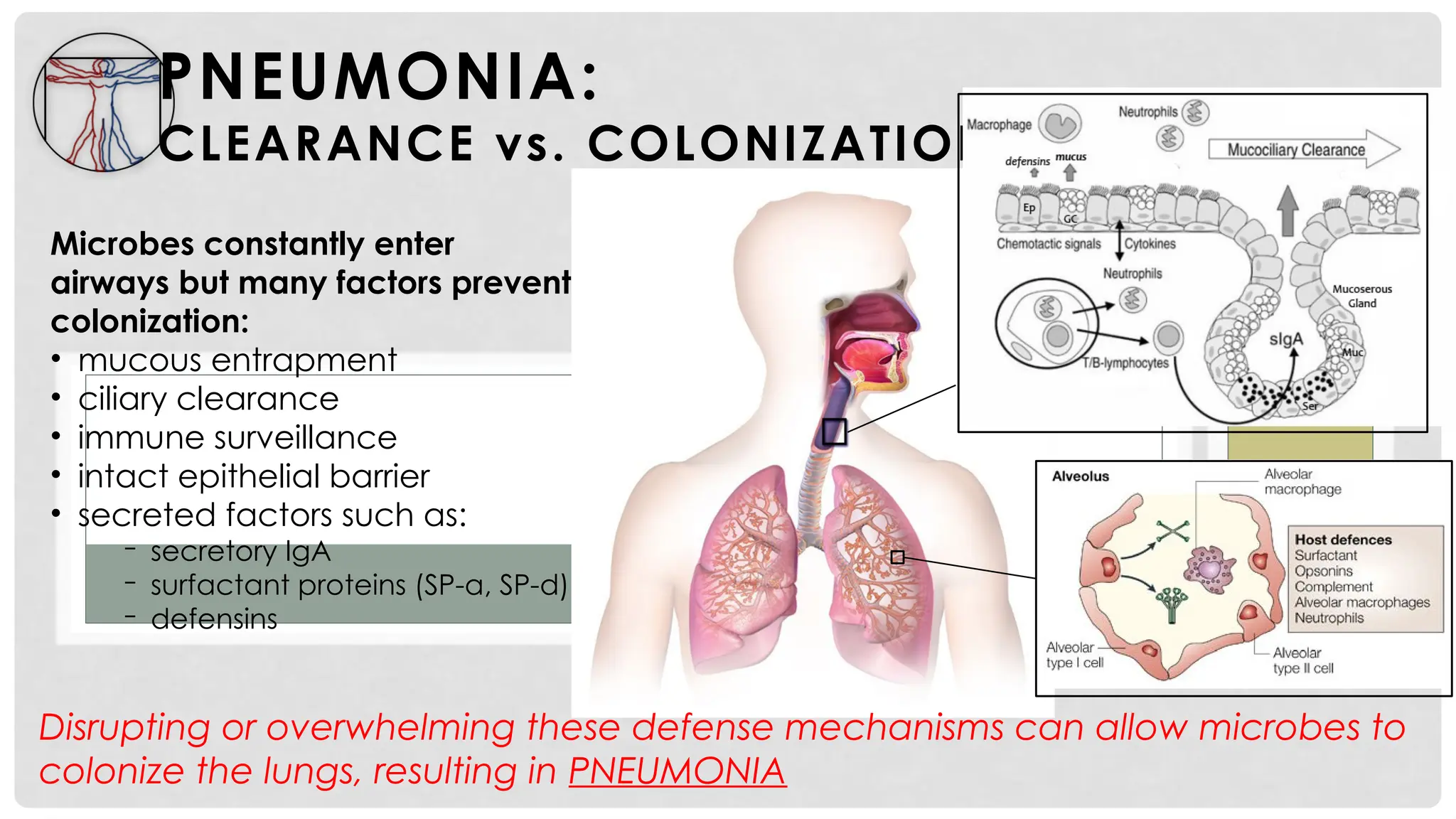
Microbesconstantly enter
airways but many factors prevent
colonization:
• mucous entrapment
• ciliary clearance
• immune surveillance
• intact epithelial barrier
• secreted factors such as:
‒ secretory IgA
‒ surfactant proteins (SP-a, SP-d)
‒ defensins
Disrupting or overwhelming these defense mechanisms can allow microbes to
colonize the lungs, resulting in PNEUMONIA
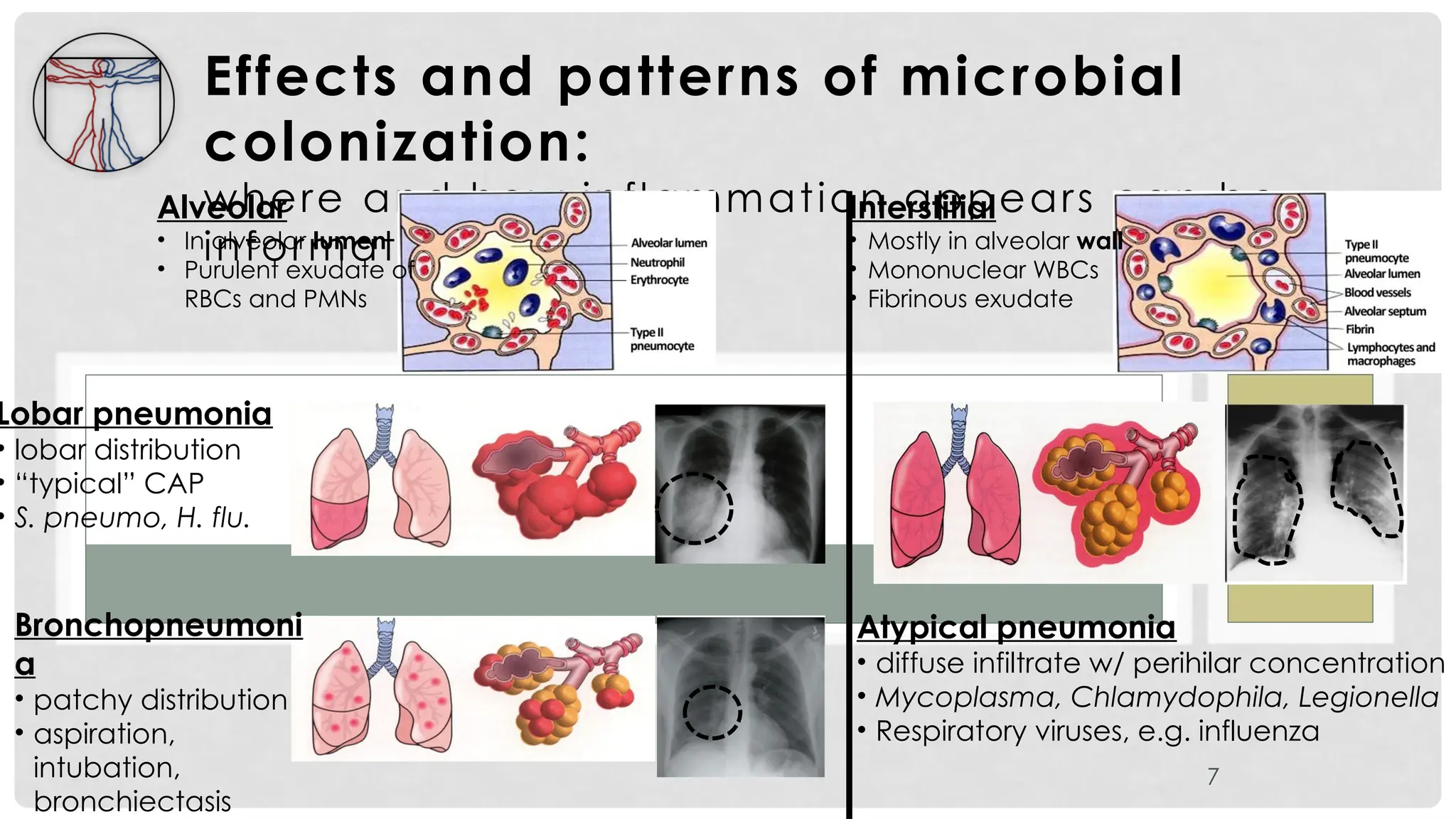
Effects and patternsof microbial
colonization:
where and how inflammation appears can be
informative
7
Alveolar
• In alveolar lumen
• Purulent exudate of
RBCs and PMNs
Interstitial
• Mostly in alveolar wall
• Mononuclear WBCs
• Fibrinous exudate
Lobar pneumonia
• lobar distribution
• “typical” CAP
• S. pneumo, H. flu.
Bronchopneumoni
a
• patchy distribution
• aspiration,
intubation,
bronchiectasis
Atypical pneumonia
• diffuse infiltrate w/ perihilar concentration
• Mycoplasma, Chlamydophila, Legionella
• Respiratory viruses, e.g. influenza
8.
8
Community-Acquired Pneumonia
• Infectionof the pulmonary parenchyma
acquired from exposure in the community
• Classically divided into “typical” and “atypical”
syndromes:
I. “Typical” CAP:
• presents with “typical” severe, acute infection
• infectious agent (usually S. pneumo or H. flu) is culturable/
identifiable
• responsive to cell-wall active antibiotics
II. “Atypical” CAP:
• presentation is usually sub-acute
9.
9
Typical CAP presentation
History
•Previously healthy with sudden onset of fever and shortness of
breath
Physical signs and symptoms
• fever
• tachycardia
• tachypnea
• productive cough with purulent sputum and possible
hemoptysis
• pallor and cyanosis
• localized:
− dullness to percussion
− decreased breath sounds
− crackles , ronchi , egophony (“E” -to-”A”
change)
Investigations
• CXR showing lobar consolidation
• CBC showing leukocytosis w/ left shift
10.
10
Typical CAP presentation
History
•Previously healthy with sudden onset of fever and shortness of
breath
Physical signs and symptoms
• fever
• tachycardia
• tachypnea
• productive cough with purulent sputum and possible
hemoptysis
• pallor and cyanosis
• localized:
− dullness to percussion
− decreased breath sounds
− crackles, ronchi, egophony (“E-to-A” change)
Investigations
• CXR showing lobar consolidation
• CBC showing leukocytosis w/ left shift
• Sputum sample contains neutrophils, RBCs; Gram stain may
11.
11
Typical CAP presentation
History
•Previously healthy with sudden onset of fever and shortness of
breath
Physical signs and symptoms
• fever
• tachycardia
• tachypnea
• productive cough with purulent sputum and possible
hemoptysis
• pallor and cyanosis
• localized:
− dullness to percussion
− decreased breath sounds
− crackles, ronchi, egophony (“E-to-A” change)
Investigations
• CXR showing lobar consolidation
• CBC showing leukocytosis w/ left shift
• Sputum sample contains neutrophils, RBCs; Gram stain may
12.
12
Atypical CAP Presentation
•32 YO healthy patient – one week of low grade
fever, sore throat, and intractable cough
• Minimal sputum production
• Able to continue to work
• No sick contacts, recent travel, or
evidence of altered immune system
• PE reveals a mildly ill-appearing patient with
diffuse wheezes on lung exam
• Primary care physician prescribes empiric
antibiotics for CAP with complete resolution
• “Walking pneumonia” syndrome
13.
13
Pleural effusion
• inflammationleads to
exudation of fluid into pleural
space
• can compromise lung function
Empyema
• purulent exudate in pleural
space
• necrosis/breakdown of visceral
pleura and/or spread of
infection into pleura
Pleural adhesions, lung fibrosis
Complications of pneumonia
14.
14
Abscess / cavitarylesion
• circumscribed focus of
liquefactive necrosis within lung
tissue
• associated with necrotizing
Staph or Strep infections or
Gram-neg rods (e.g. aspiration)
Complications of pneumonia
15.
15
Credits: Pneumonia
Location ofitem (slide #5): "Respiratory system complete no labels" by Bibi Saint-Pol -
en.wikipedia.org/wiki/File:Respiratory_system_complete_en.svg. Licensed under CC BY-SA 3.0 via
Wikimedia Commons
http://commons.wikimedia.org/wiki/File:Respiratory_system_complete_no_labels.svg#/media/File:Respirat
ory_system_complete_no_labels.svg
Location of item (slide #5): "Diagram showing a build up of fluid in the lining of the lungs (pleural effusion)
CRUK 054" by Cancer Research UK - Original email from CRUK. Licensed under CC BY-SA 4.0 via Wikimedia
Commons -
http://commons.wikimedia.org/wiki/File:Diagram_showing_a_build_up_of_fluid_in_the_lining_of_the_lungs
_(pleural_effusion)_CRUK_054.svg#/media/File:Diagram_showing_a_build_up_of_fluid_in_the_lining_of_the
_lungs_(pleural_effusion)_CRUK_054.svg
Location of item (slide #5): Bronchitis illustration: http://commons.wikimedia.org/wiki/File:Bronchitis.jpg --
This work is in the public domain in the United States because it is a
work prepared by an officer or employee of the United States Government as part of that person’s official
duties
under the terms of Title 17, Chapter 1, Section 105 of the US Code.
Location of item (slide #6): color illustration of upper and lower airway anatomy. Blausen.com staff. "
Blausen gallery 2014". Wikiversity Journal of Medicine.DOI:10.15347/wjm/2014.010. ISSN 20018762. - Own
work
16.
16
Credits (continued): Pneumonia
Locationof item (slide #6): illustration of alveolar defense mechanisms.
http://www.nature.com/nri/journal/v5/n1/fig_tab/nri1528_F1.html. Figure 1 from Wright, JR.
Immunoregulatory functions of surfactant proteins. Nat Rev Immunol. 2005; 5: 58-68.
doi:10.1038/nri1528
Location of item (slide #7): color illustrations of alveolar and interstitial inflammation, lobar, bronchial,
and interstitial patterns of pneumonia.
http://quizlet.com/27416956/pulmonary-pathology-and-pathophysiology-flash-cards/. Contributors
to Quizlet.com warrant that the downloading, copying and use of the content will not infringe the
proprietary rights, including but not limited to the copyright, patent, trademark or trade secret rights,
of any third party.
Location of item (slide #7 and slide #12): chest x-ray of lobar pneumonia.
http://biomarker.cdc.go.kr/biomarker/diseaseimg/pneumonia-Community_acquired.jpg
Location of item (slide #7): chest x-ray of bronchopneumonia.
http://www.ebmedicine.net/topics.php?paction=showTopicSeg&topic_id=118&seg_id=2306
Location of item (slide #7): chest x-ray of interstitial (atypical) pneumonia.
http://www.ebmedicine.net/topics.php?paction=showTopicSeg&topic_id=118&seg_id=2306
Location of item (slide #11): illustration of CAP patient. RWJF Pneumonia Module Springboard Video.
17.
17
Credits (continued): Pneumonia
Locationof item (slide #11): crackles sound clip: http://en.wikipedia.org/wiki/File:Crackles_pneumoniaO.ogg;
ronchi sound clip: http://www.easyauscultation.com/cases?coursecaseorder=5&courseid=201; normal “E” lung
sound: http://www.easyauscultation.com/cases?coursecaseorder=4&courseid=202; egophony lung sound (“E”
to “A” change): http://www.easyauscultation.com/cases.aspx?coursecaseorder=5&courseid=202
Location of item (slide #13): Gram Stain of a film of sputum from a case of lobar pneumonia. CDC
Location of item (slide #14 & 15): Chest X-ray of atypical pneumonia. Dr. Mike Malinzak. Duke University. Dept. of
Radiology.
Location of item (slide #16): Chest X-ray of HAP. Dr. Mike Malinzak. Duke University. Dept. of Radiology.
Location of item (slide #17): "Diagram showing a build up of fluid in the lining of the lungs (pleural effusion) CRUK
054" by Cancer Research UK - Original email from CRUK. Licensed under CC BY-SA 4.0 via Wikimedia Commons -
http://commons.wikimedia.org/wiki/File:Diagram_showing_a_build_up_of_fluid_in_the_lining_of_the_lungs_(pleur
al_effusion)_CRUK_054.svg#/media/File:Diagram_showing_a_build_up_of_fluid_in_the_lining_of_the_lungs_(pleura
l_effusion)_
CRUK_054.svg
Location of item (slide #18): "CT chest in pneumonia with abscesses caverns and effusions d0" by Christaras A -
Own work from anonmyized dicom image. Licensed under CC BY 2.5 via Wikimedia Commons -
http://commons.wikimedia.org/wiki/File:CT_chest_in_pneumonia_with_abscesses_caverns_and_effusions_d0.jpg
#/media/File:CT_chest_in_pneumonia_with_abscesses_caverns_and_effusions_d0.jpg



























![Pulmonary_inections[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonaryinections1-230718060523-80803fef-thumbnail.jpg?width=640&height=640&fit=bounds)






































