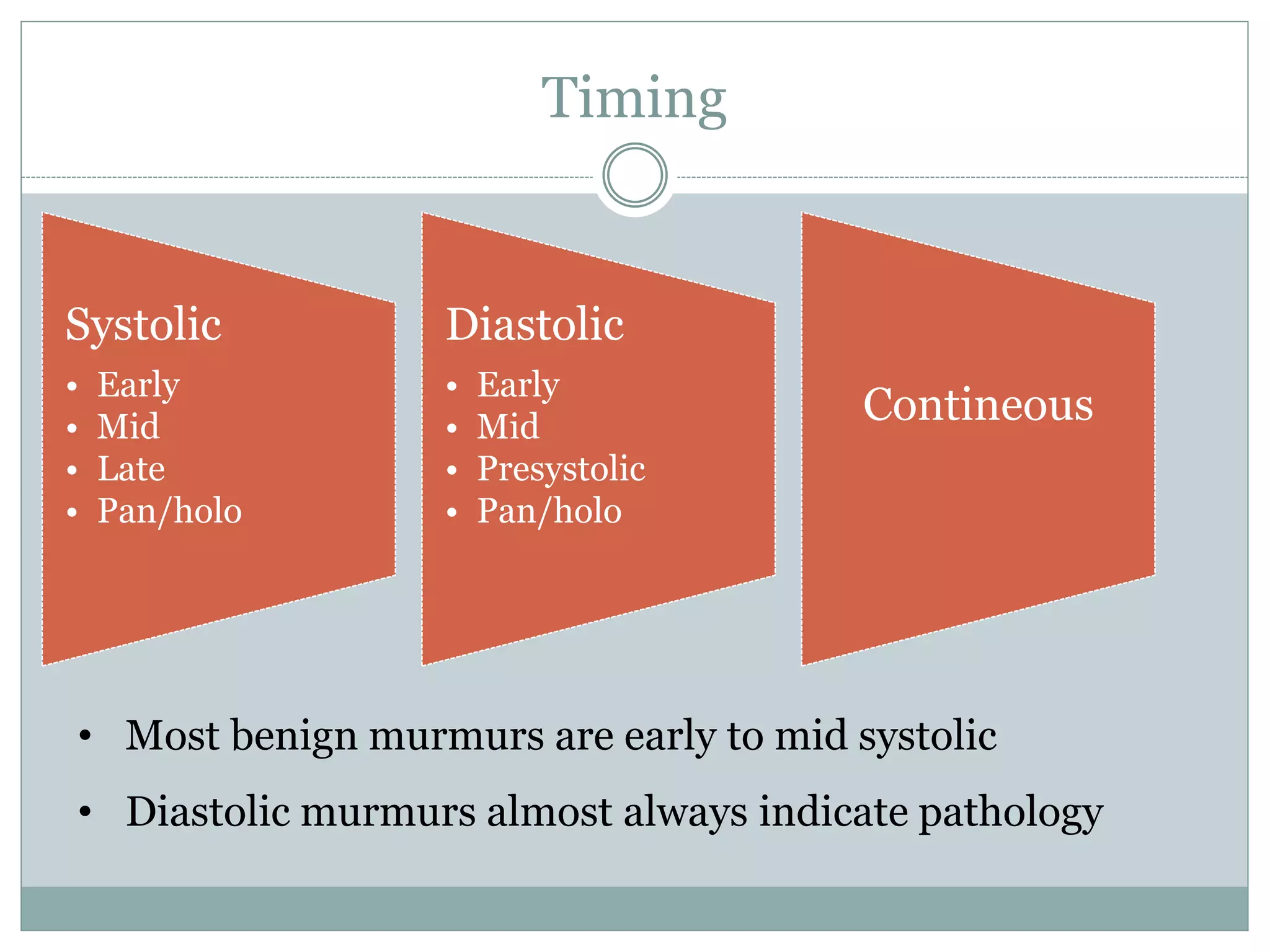
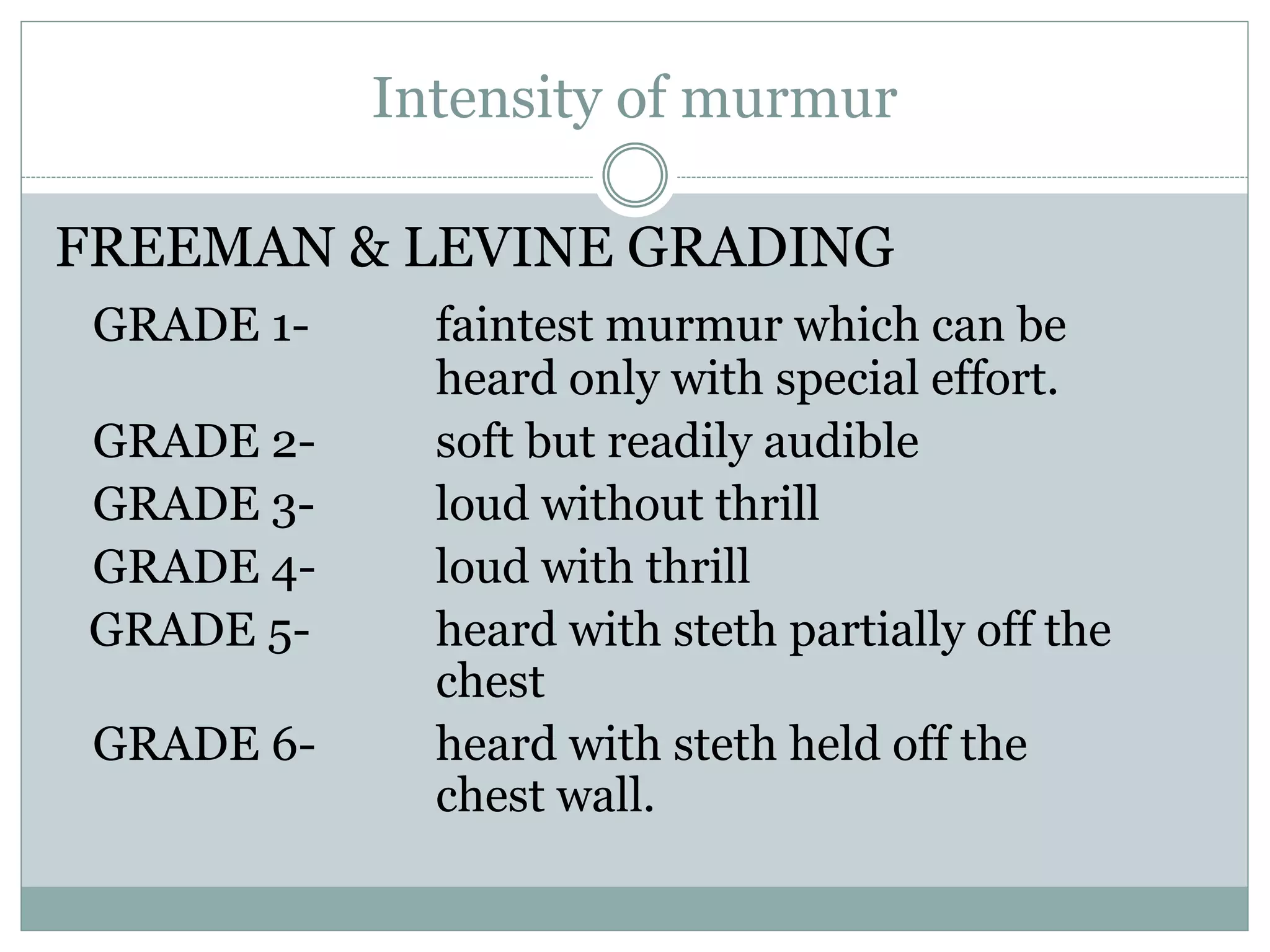
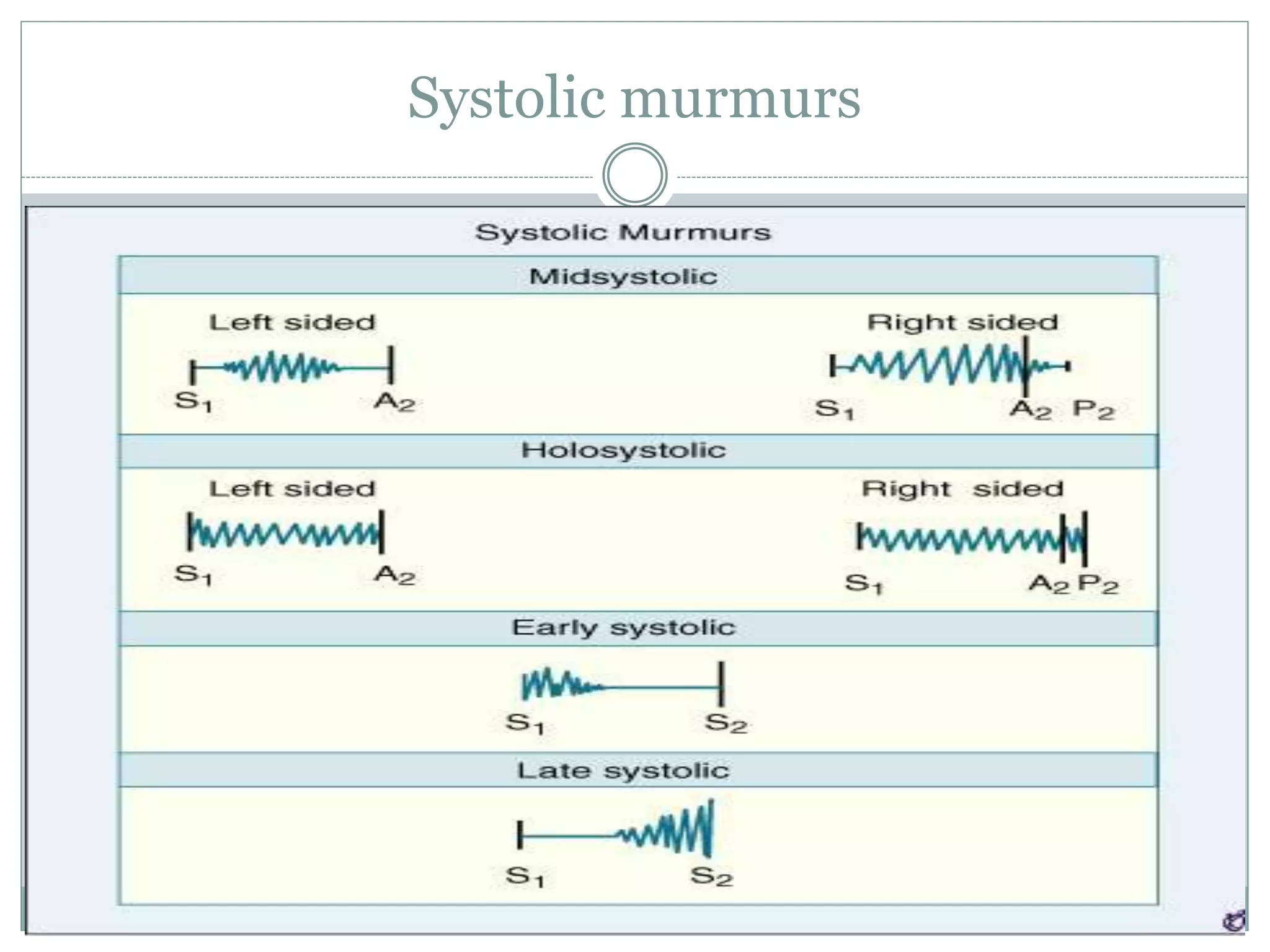
This document discusses the approach to heart murmurs. It defines a murmur and describes how they are produced. It outlines the key aspects for describing a murmur, including timing, location, intensity, quality, transmission, and configuration. The main types of murmurs are discussed - systolic (early, mid, late), diastolic, and continuous. The most common causes of each type are explained along with distinguishing characteristics. Physiological murmurs are also reviewed. The document provides guidance on performing a thorough exam and analysis to determine the cause and significance of a heart murmur.















![AS
MR AS [ Gallaverdin]
Apical mid sys/
Holosystolic
Apical mid sys
A2 buried in late sys
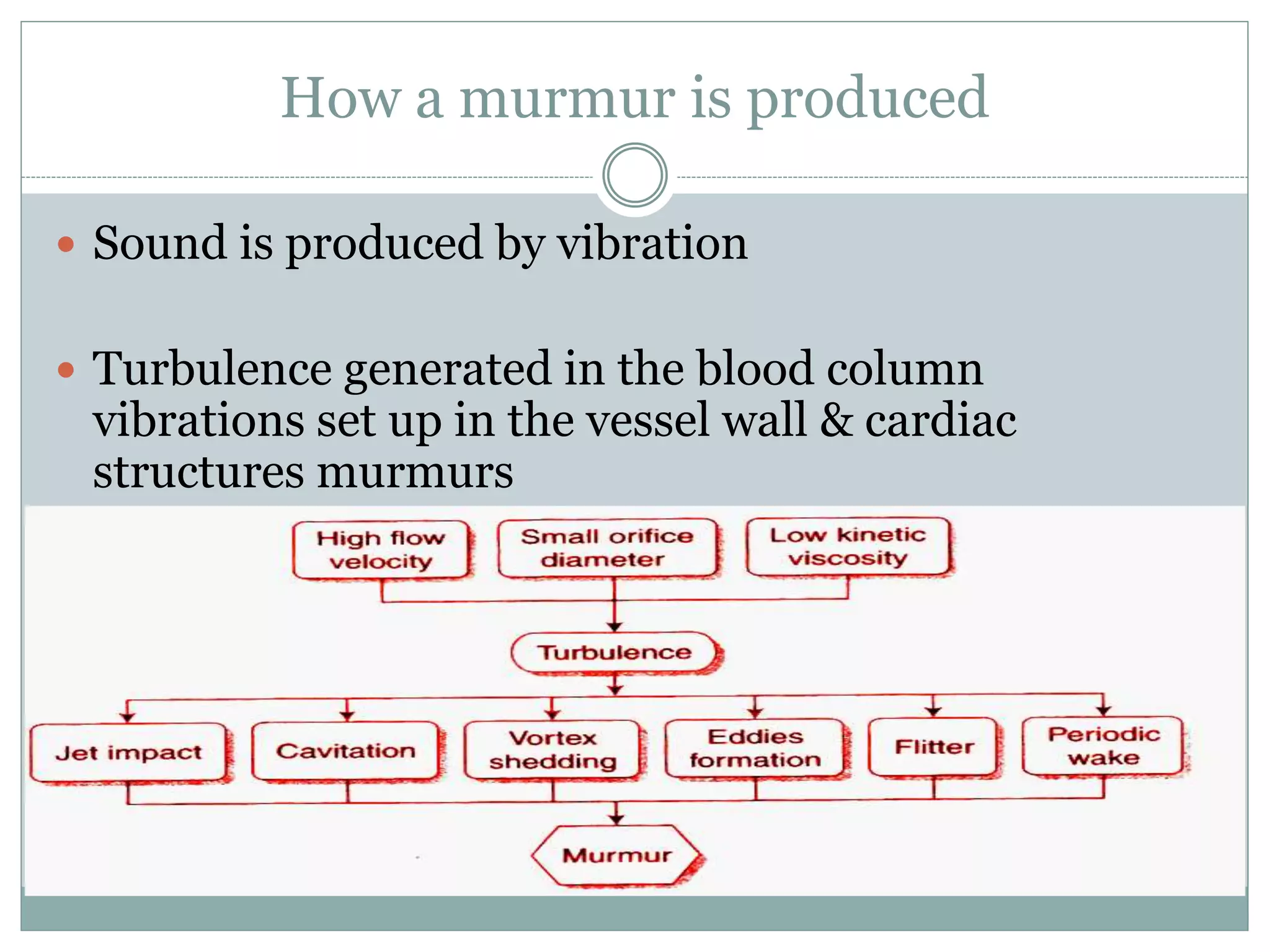
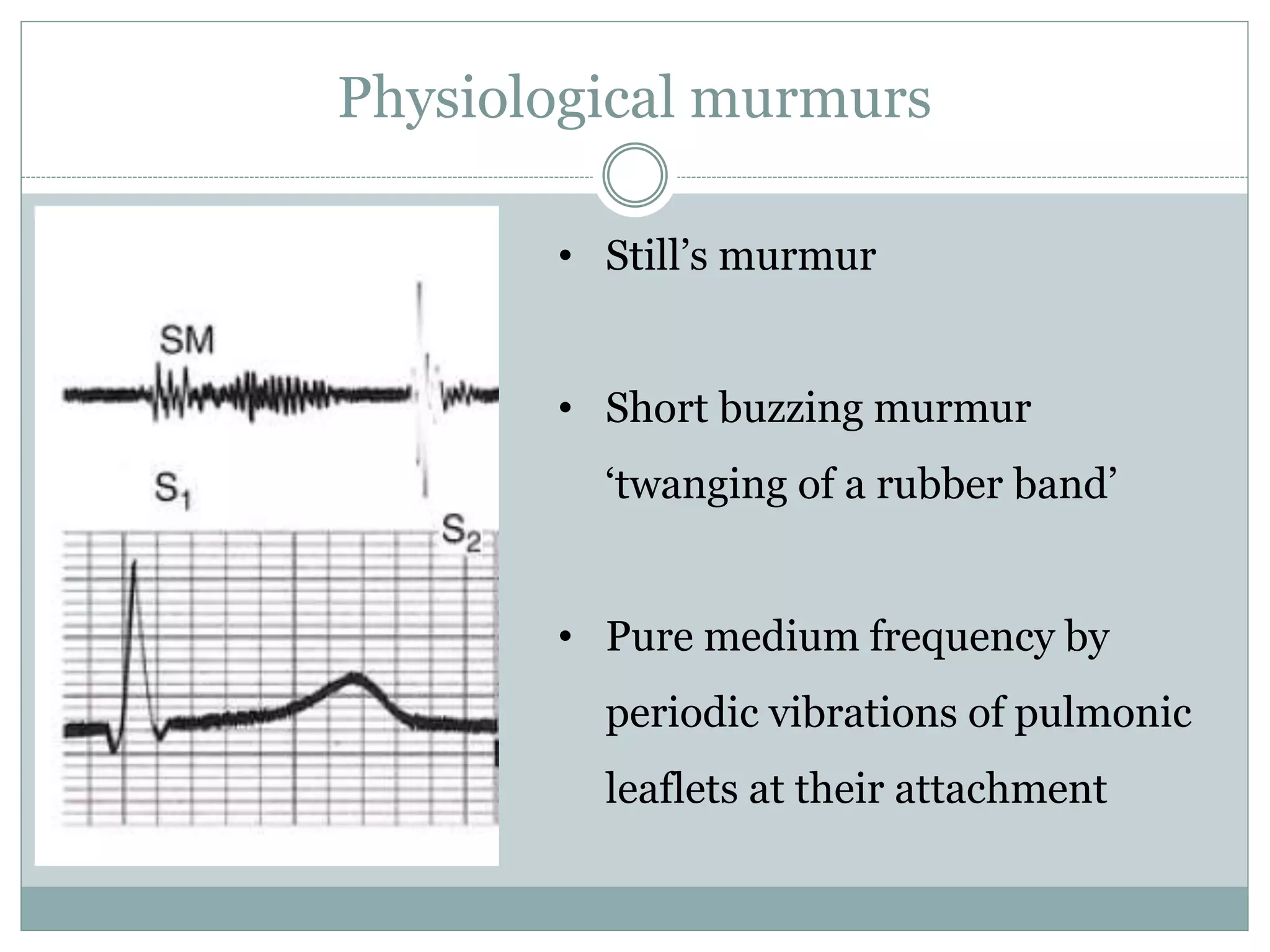
vibrations
Clear S2 heard
P/PVC unchanged P/PVC mur =
Amyl nitrate = Amyl nitrate =
Pulse normal Pulsus parvus et
tardus
Gallaverdin phenomenon/ hourglass
phenomenon
Lower n (aortic) vs. Higher n (mitral)
periodic vibrations of stiffened non calcific
aortic valve
Differentiating from MR](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-24-2048.jpg)











![Mammary Soufflé
• Late Pregnancy or puerperium
• Sometimes continuous louder in
systole, distinct gap from S1 [ time
for ejected blood to reach
mammary arteries]
• 2 or 3 RICS/ LICS
• Light Pressure augments murmur
becomes continuous; firm Pr
abolishes murmur](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-38-2048.jpg)
![Late systolic murmurs
MVP
• Leaflets remains competent during early
ventricular contraction but overshoot in late
systole [critical V. dimensions]
• One or more mid systolic clicks precede murmur
[sudden deceleration of the column of blood
against the prolapsed leaflet or scallops]
• Longer and softer
• Prompt standing after squatting
• Valsalva II
• Short & louder
• squatting
• Sustained hand grip
• Amyl nitrate
Barlow’s syndrome refers to the
spectrum of symptoms caused by
MVP [click or murmur alone to
palpitations, chest pain, or syncope]](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-39-2048.jpg)














![Mitral stenosis
• Low n rough rumbling [sound of
distant thunder] MDM
• Localized to apex, better heard in
left lateral position with bell
• Length a severity
• Long murmurs up to S1 even in
long cycles of AF- severe MS
• Late diastolic or Pre systolic
accentuation usually seen in
pliable valves and in NSR [
sometimes in AF]](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-56-2048.jpg)
![TS
Similar to MS
Murmur usually seen associated with AF
Diff. from MS
Increases during inspiration [Augmentation of RV volume, RV
Diastolic Pr., Flow rate and gradient across valve]
LLSB](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-57-2048.jpg)


![Other Mid Diastolic Murmur
Carey Coomb’s murmurs
Acute rheumatic fever, mitral valve structures acutely inflamed with
some thickening and edema turbulence of flow during the rapid
filling phase.
+ moderate MR [increased mitral inflow in diastole]
Low pitched short MDM.
good evidence of active carditis](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-60-2048.jpg)

![Late Diastolic/ Pre-systolic Murmurs
MS
Higher frequency than MDM
Sometimes only PSA heard- mild MS
Generally absent in calcified valves and most of AF [
may be present during short cycle lengths in AF]
Cause-
Increased flow during atrial contraction in late systole
Increased dp/dt of LV contraction increases turbulence [ esp.
in AF short cycles]](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-62-2048.jpg)
![Other diastolic murmurs
Cabot– Locke Murmur- [Diastolic Flow murmur]
The Cabot–Locke murmur is a diastolic murmur that sounds similar to
aortic insufficiency but does not have a decrescendo; it is heard best at the
left sternal border. [High flow thru coronary vessels, LMCA, LAD]
The murmur resolves with treatment of anaemia.
Dock’s murmur
diastolic crescendo-decrescendo, with late accentuation, [consistent with
blood flow through the coronary] in a sharply localized area, 4 cm left of the
sternum in the 3LICS, detectable only when the patient was sitting upright.
Due to stenosis of LAD](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-63-2048.jpg)
![ Key–Hodgkin murmur
EDM of AR; it has a raspy quality, [sound of a saw cutting through wood]. Hodgkin
correlated the murmur with retroversion of the aortic valve leaflets in syphilitic disease.
Rytand’s murmur in complete heart block
MDM or Late diastolic murmur
Atrial contraction coincides with the phase of rapid diastolic filling increased flow short
MDM [intermittent].
Another theory- Delayed V. contraction following A. contraction may lead to diastolic MR &
TR, because AV valve closure does not occur [unless V. systole supervenes]. When higher V
than A pressure during atrial relaxation, an incompletely closed AV valve may lead to a
reverse gradient with a considerable regurgitation volume.](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-64-2048.jpg)



![Continuous murmurs
APW
2 or 3 LICS
Usually associated with early devp of eissenmenger
RSOV
No peaking at S2 seen [peaks in sys or dia.]
To RA- RLSB
RV- LLSB
RVOT- 3 LICS
Lutembacher syndrome with restricted ASD
LLSB [body of RA]](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-68-2048.jpg)
![Continuous murmurs
C-AVF
RA- RLSB or RUSB
CS- back b/w spine & Lt scapula
RV inflow- LLSB
RVOT- Upper to Mid LSB [beat to beat change in murmur may be present,
RV systolic compression, valsalva softens murmur]
PA- ULSB [no eddy sounds]
ALCAPA
Murmur louder in diastole [LV contr. I/C flow]
Do not peak at S2
Usu LUSB or RUSB
o LA- ULSB rad to Lt ant ax line
o Lt SVC- upper to mid LSB](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-69-2048.jpg)


![Position
A. Lt Lateral Decubitus
LV impulse [apical sounds, murmurs better heard]
Act of turning increases HR[ MDM & PSA of MS ],
induces PVC [AS murmur vs. MR murmur (n/c)]
B. Sitting leaning forward full held expiration
AR & PR EDM
C. Sitting with legs dangling
Further reduces venous return
If S2 fails to fuse on sitting
D. Elbow Knee Position
Pericardial friction rub](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-72-2048.jpg)
![Position
E. Standing to squatting and vice versa
Standing[ venous return, BP ]; [opp. in squatting]
1. All murmurs [ except HOCM , MVP earlier]
HOCM [ LV contractility, after load, preload]
MVP [ preload, afterload ]
2. A2- P2 , A2-OS , A2-S3 (n/c)
F. Hyperextension of shoulders
supraclavicular Systolic murmurs
G. Stretching of Neck
Venous hum
H. Passive elevation of both legs
Transiently increases venous return, increase S3](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-73-2048.jpg)
![Physical Maneuvers
Inspiration
Right sided events become
more prominent
S2 split appreciable
RVs3 RVs4 prominent
Tricuspid sys & dia Mur
increased
Pulm ejection sound
reduced
Expiration
• Left sided events become
more prominent
• Diff AR & PR
• Pericardial friction rub
[exhalation & supine]
• Innocent pulm mid sys
murmur becomes more
prominent becos of
reduced AP diameter](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-74-2048.jpg)






![Pharmacological Maneuvers
Inhalation of Amyl Nitrate [Crush ampoule in towel, 3-4 deep
breaths over 10–15 s]
Lasts 2 minutes
No reduction in stroke volume as seen in NTG
First 30 secs 30 to 60 secs > 60 secs
Decreased Sys Art
Pressure
Reflex Tachycardia Increased CO, HR](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-81-2048.jpg)
![Amyl Nitrate inhalation
AS vs. MR
TR vs. MR
PS vs. TOF
MS vs. Austin F
PR vs. AR
HOCM vs. MVP [n/c]](https://image.slidesharecdn.com/approachtoheartmurmurs-220618164539-0ca03cd7/75/Approach-to-Heart-Murmurs-pptx-82-2048.jpg)







































![[Int. med] heart murmurs from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/b29t6cwrtzwunmrfazue-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171700-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)



































