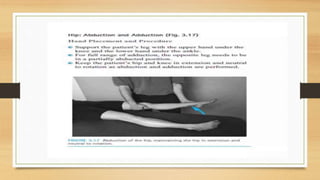
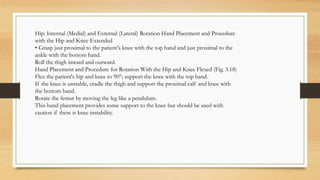
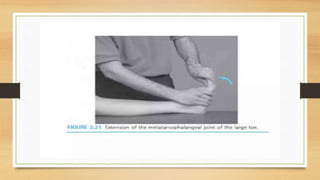
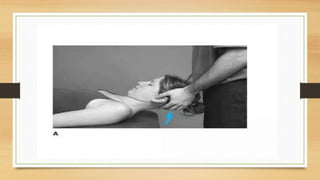
This document provides information about joint mobility techniques for various joints of the body. It begins with definitions of joint mobility and common causes of limited mobility. It then describes techniques for assessing and improving range of motion in major joints like the shoulder, elbow, wrist, hip, knee, ankle, cervical spine, and lumbar spine. Diagrams show hand placement and procedures for passive range of motion exercises targeting specific motions, like flexion, extension, lateral flexion, and rotation. The goal is to safely increase range of motion and maintain or restore mobility.





























































![J._CONTRAST_BATH_THERAPY[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/j-230713132551-5c45004c-thumbnail.jpg?width=640&height=640&fit=bounds)





































![INJURIES AROUND HIP [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/injuriesaroundhipautosaved-240206110505-4ae81da1-thumbnail.jpg?width=640&height=640&fit=bounds)





















