Downloaded 209 times




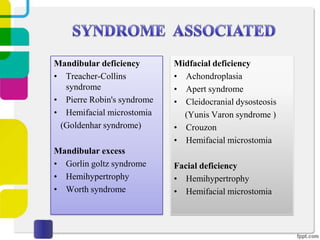
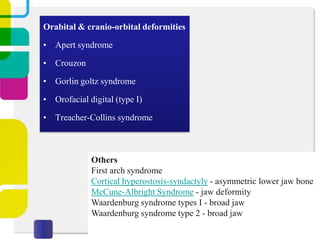
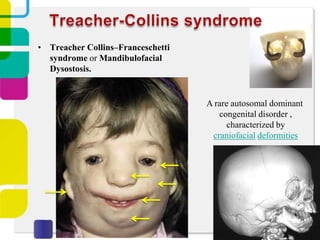
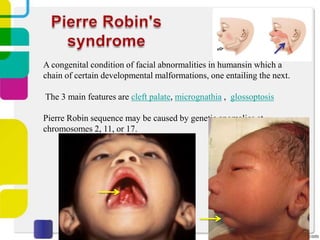
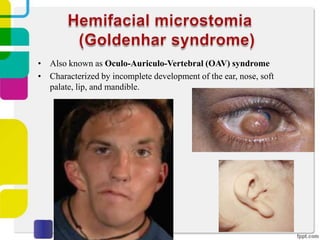
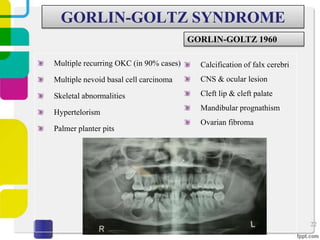

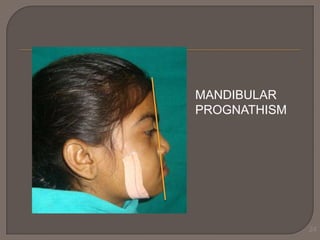


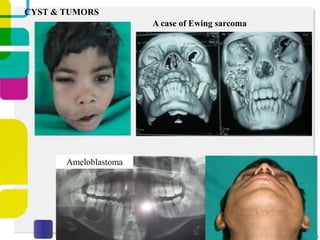
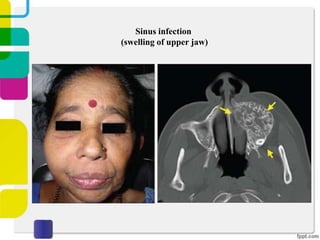






This document discusses jaw deformities including their definition, history, classification, treatment considerations, and complications. It provides details on congenital and acquired causes such as trauma during birth, wisdom tooth removal, and infections. Specific conditions that can cause jaw deformities like Treacher Collins syndrome and Pierre Robin sequence are explained. The treatment of early jaw deformity cases and development of procedures like Le Fort osteotomies are summarized.











































































































