Downloaded 28 times

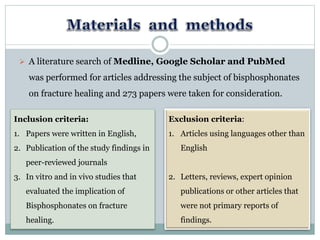

The document summarizes research on how bisphosphonates affect fracture healing. Bisphosphonates are commonly used to treat osteoporosis but their long-term use may delay fracture healing in some cases. Studies in humans found no effect on healing in most patients, but those using bisphosphonates long-term (over 10 years) showed delayed healing in about 26% of cases. Animal studies also suggest long-term bisphosphonate use may impair healing. The document reviews evidence from both human and animal studies on the implications of bisphosphonate use for fracture recovery.





























































































