











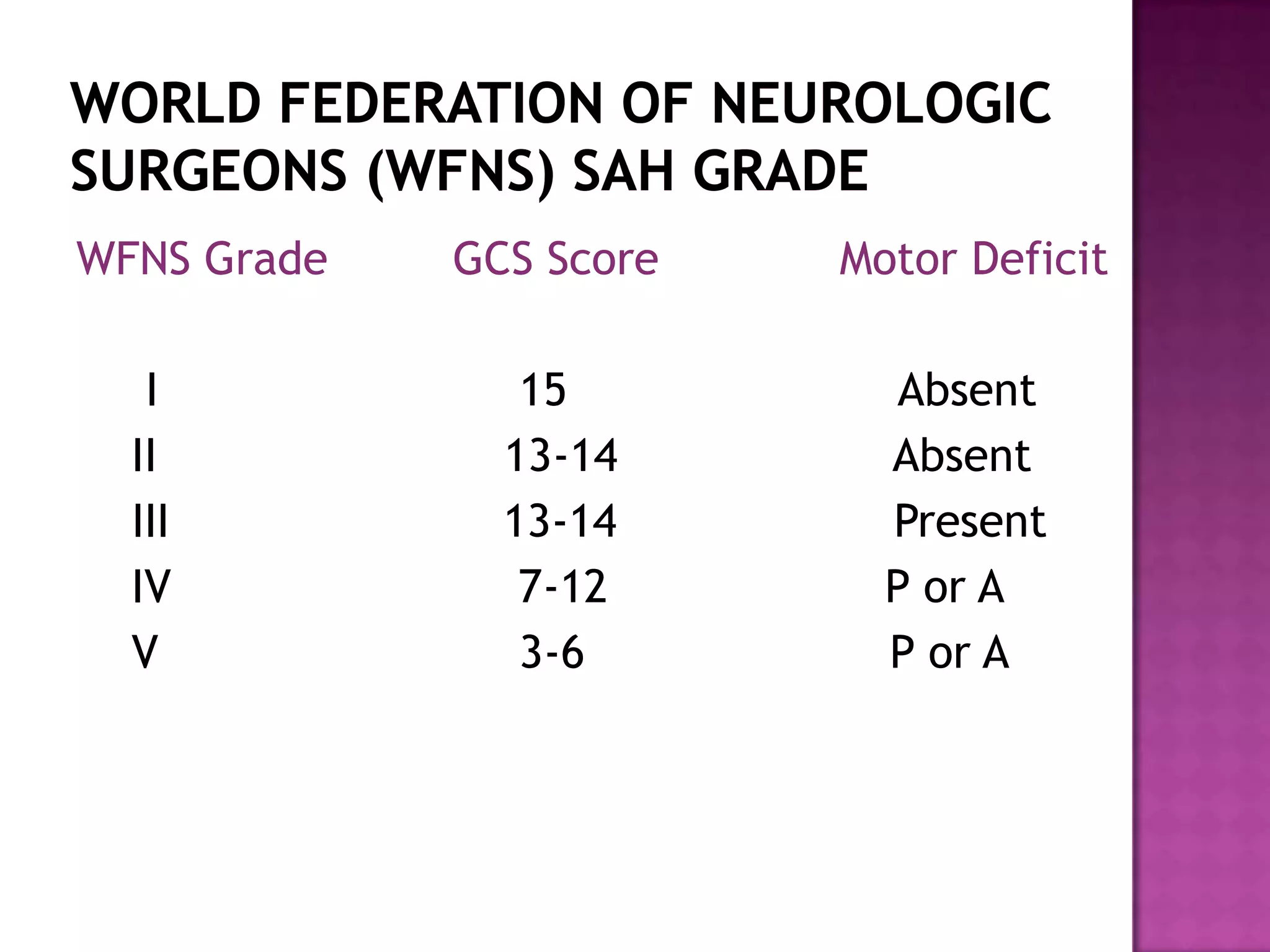


























































This document discusses cerebral aneurysms and subarachnoid hemorrhage. It provides details on: - The incidence, risk factors, locations, and causes of cerebral aneurysms - Grading scales used to assess the severity of subarachnoid hemorrhage - Complications associated with subarachnoid hemorrhage such as vasospasm, rebleeding, and elevated intracranial pressure - Management strategies for unruptured and ruptured aneurysms including surgical clipping and endovascular coiling to prevent rebleeding

![Anesthetic management of carotid endarterectomy [autosaved] 2](https://cdn.slidesharecdn.com/ss_thumbnails/anestheticmanagementofcarotidendarterectomyautosaved2-170323192218-thumbnail.jpg?width=640&height=640&fit=bounds)






























































![Anaesthesia for intracranial aneurysm clipping[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anaesthesiaforintracranialaneurysmclipping1-250918124339-735bae7b-thumbnail.jpg?width=640&height=640&fit=bounds)





















