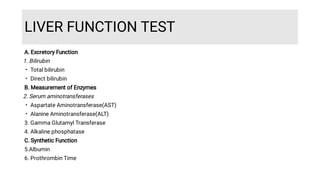
1. Liver function tests evaluate the liver's excretory, synthetic, and biochemical functions through markers like bilirubin, aminotransferases, alkaline phosphatase, albumin, and prothrombin time.
2. Elevated aminotransferases indicate hepatocellular injury from factors like viral hepatitis, drugs, or ischemia. Alkaline phosphatase is elevated in cholestatic conditions from intrahepatic or extrahepatic bile duct obstruction. Albumin and prothrombin time reflect synthetic function.
3. Interpreting liver function tests involves considering the pattern of marker elevations, clinical history of exposures, and additional tests to determine the specific cause and severity of liver disease.












































![L8-Liver_Function_Test[1] SF.pptbwdqdbdwub](https://cdn.slidesharecdn.com/ss_thumbnails/l8-liverfunctiontest1sf-250507164033-55d694e3-thumbnail.jpg?width=640&height=640&fit=bounds)




































