Downloaded 154 times


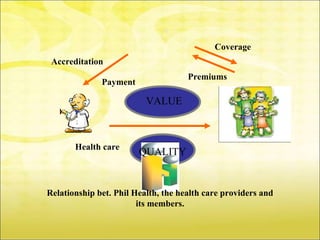

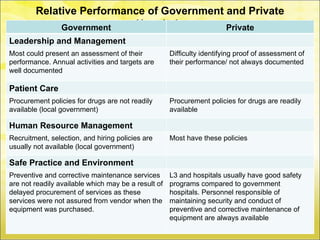
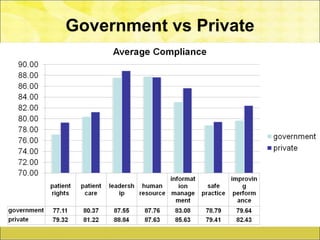
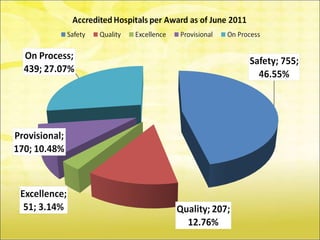



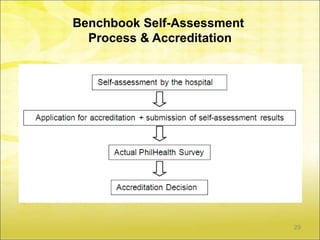








The document discusses implementing a quality assurance program through accreditation, health technology assessment, peer review, feedback mechanisms, and performance monitoring. It outlines PhilHealth's accreditation of different types of healthcare providers like physicians, hospitals, rural health units, and more. Minimum requirements for accreditation include 100% compliance with core indicators and 60% compliance in key areas like patient rights, care, and safety for centers, or 75% compliance in additional areas like leadership for assistant centers. The document emphasizes continuous quality improvement.



















































![Hospital licensing process_up_cph[1]](https://cdn.slidesharecdn.com/ss_thumbnails/hospitallicensingprocessupcph1-120603011737-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Legal aspects up hospital administrators lect[1]](https://cdn.slidesharecdn.com/ss_thumbnails/legalaspectsuphospitaladministratorslect1-120603011330-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)































