Download as PPSX, PPTX
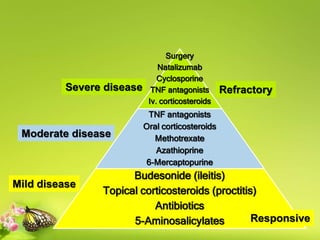
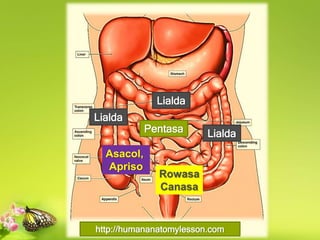

This document summarizes aminosalicylates, a class of drugs used to treat inflammatory bowel disease. It describes how various formulations like sulfasalazine, olsalazine, and mesalamine compounds deliver the active drug 5-aminosalicylic acid to different parts of the gastrointestinal tract. It also discusses the pharmacokinetics, pharmacodynamics, clinical uses, and potential adverse effects of aminosalicylates.













































![INFLAMATORY BOWEL DISORDER [IFD] .ppt](https://cdn.slidesharecdn.com/ss_thumbnails/inflamatoryboweldisorder-250605044139-61f49cba-thumbnail.jpg?width=640&height=640&fit=bounds)





















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



