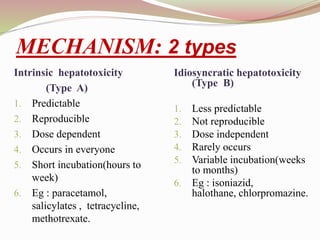
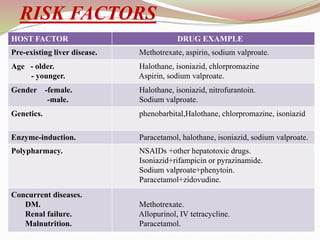
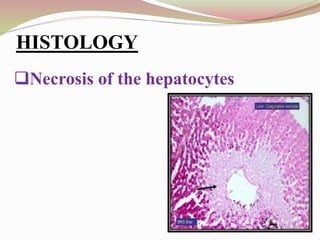
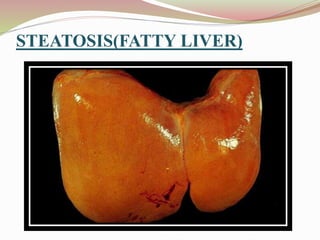
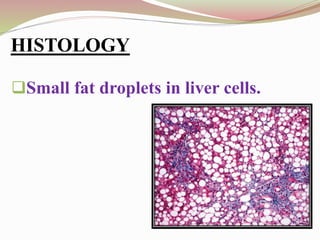
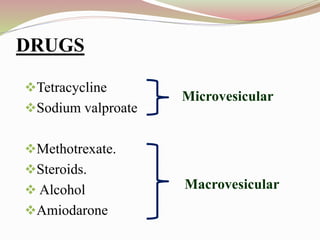
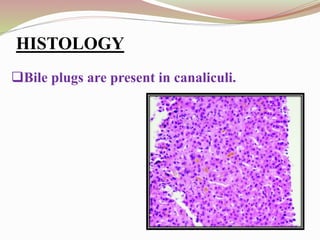
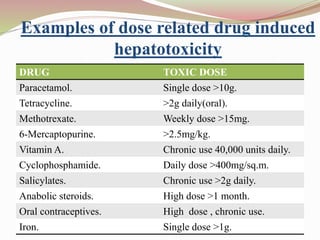
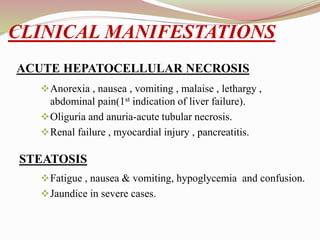
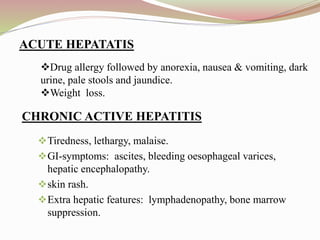
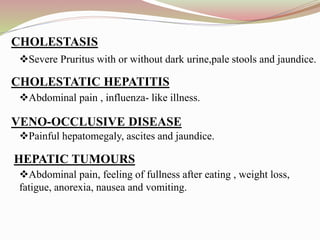
This document provides an overview of drug-induced liver disease (DILD). It defines DILD and discusses its epidemiology and risk factors. Two main mechanisms of hepatotoxicity are described - intrinsic and idiosyncratic. Various types of DILD are outlined including hepatocellular necrosis, steatosis, cholestasis, granulomatous hepatitis, and fibrosis/cirrhosis. Clinical manifestations, investigations, and treatment approaches are summarized. Assessment involves a patient history, liver enzyme levels, biopsy, and nutritional status evaluation. Treatment focuses on diagnosis, drug withdrawal, supportive care, and use of antidotes/corticosteroids if needed.






































![Acute and chronic liver disease [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/acuteandchronicliverdiseaseautosaved-250921172441-4babef2c-thumbnail.jpg?width=640&height=640&fit=bounds)













![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















