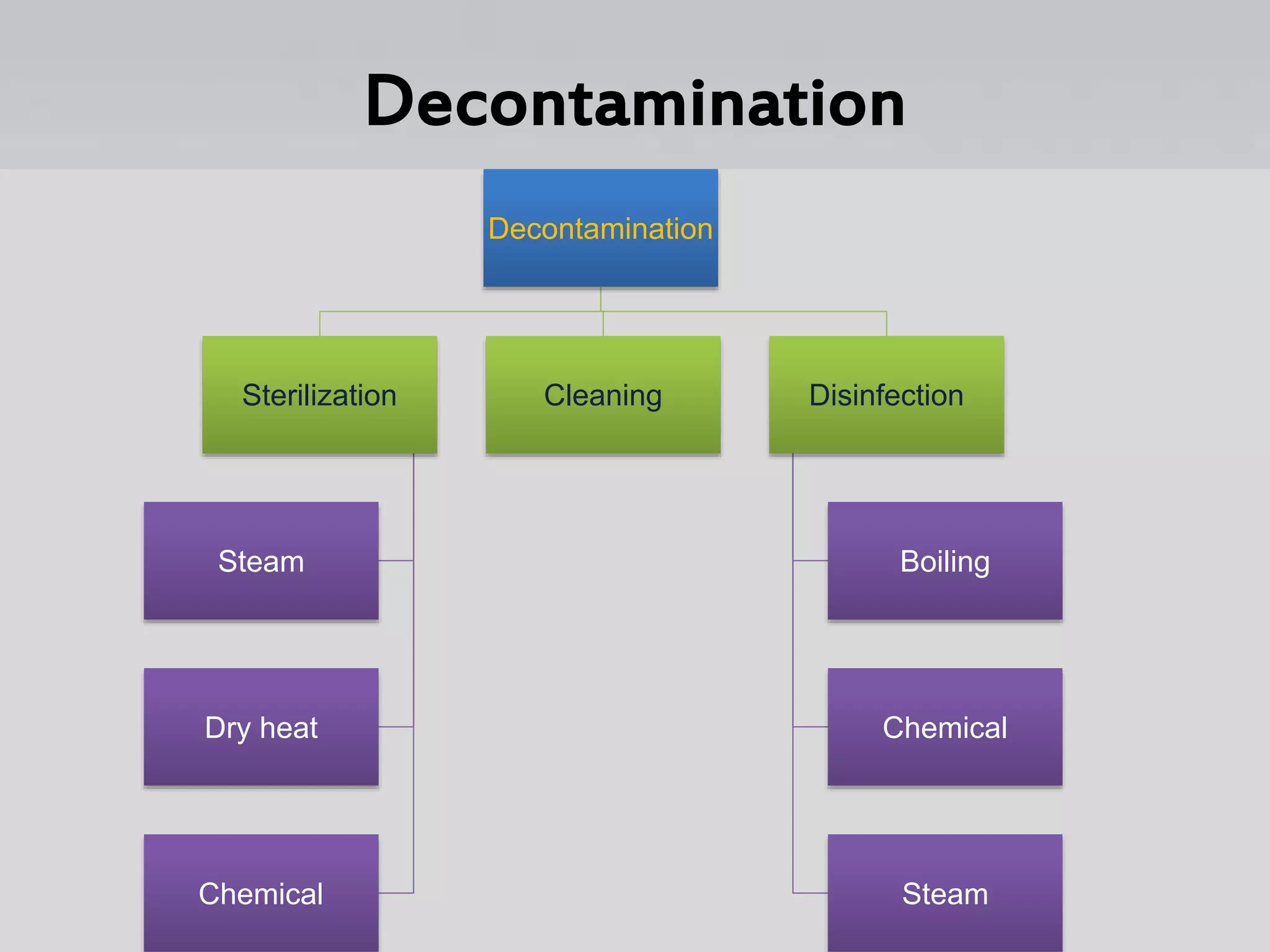
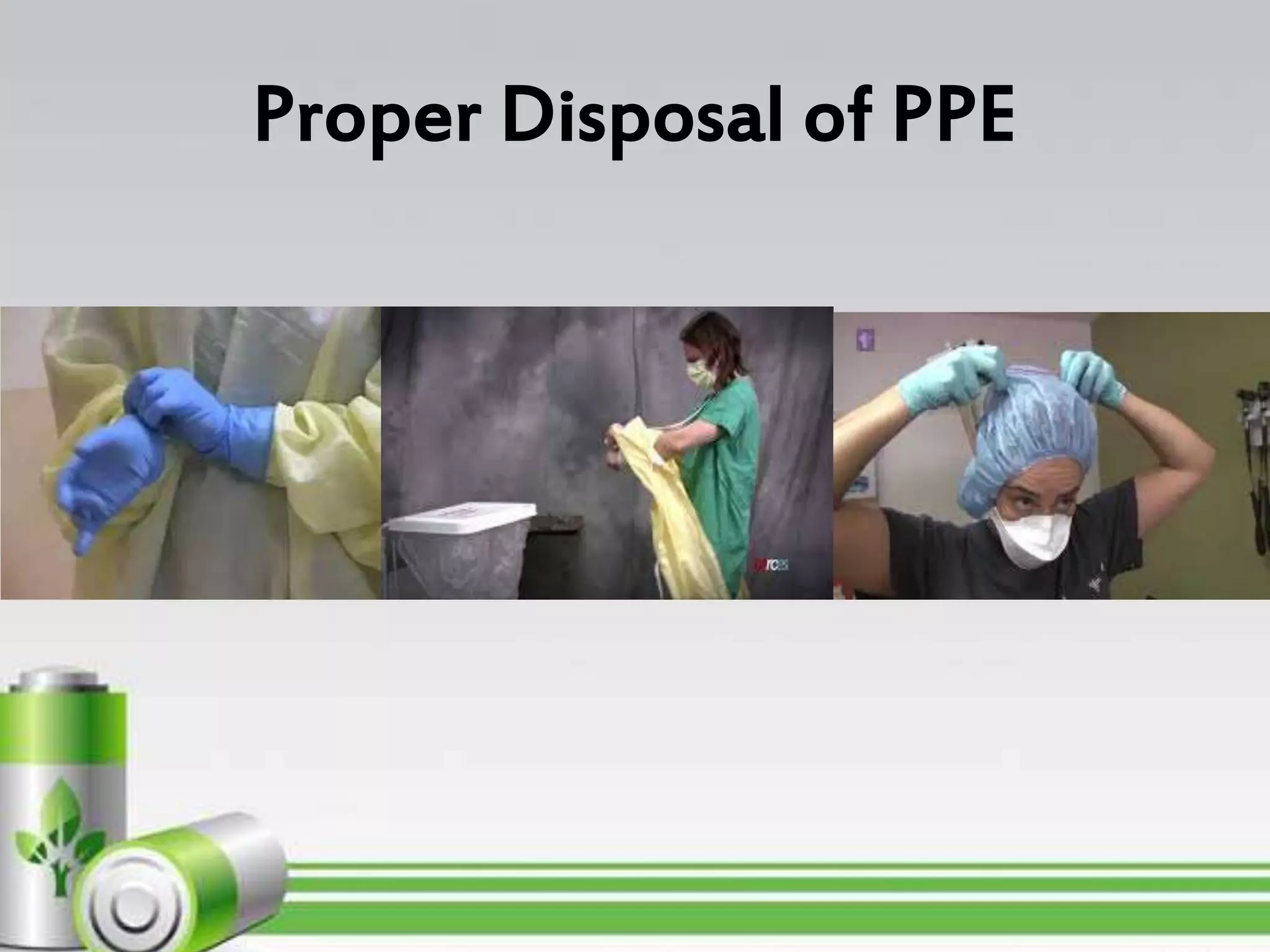
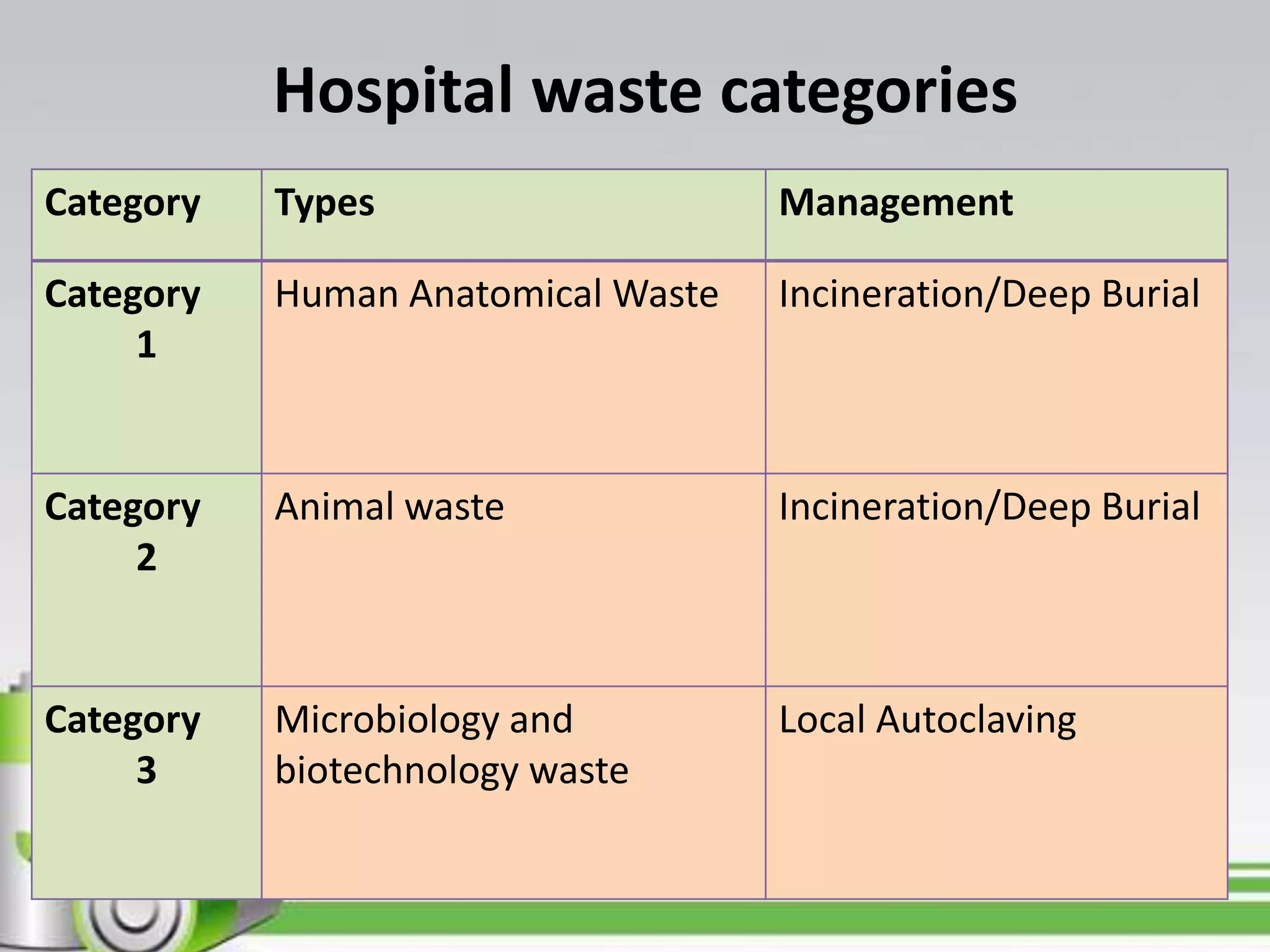
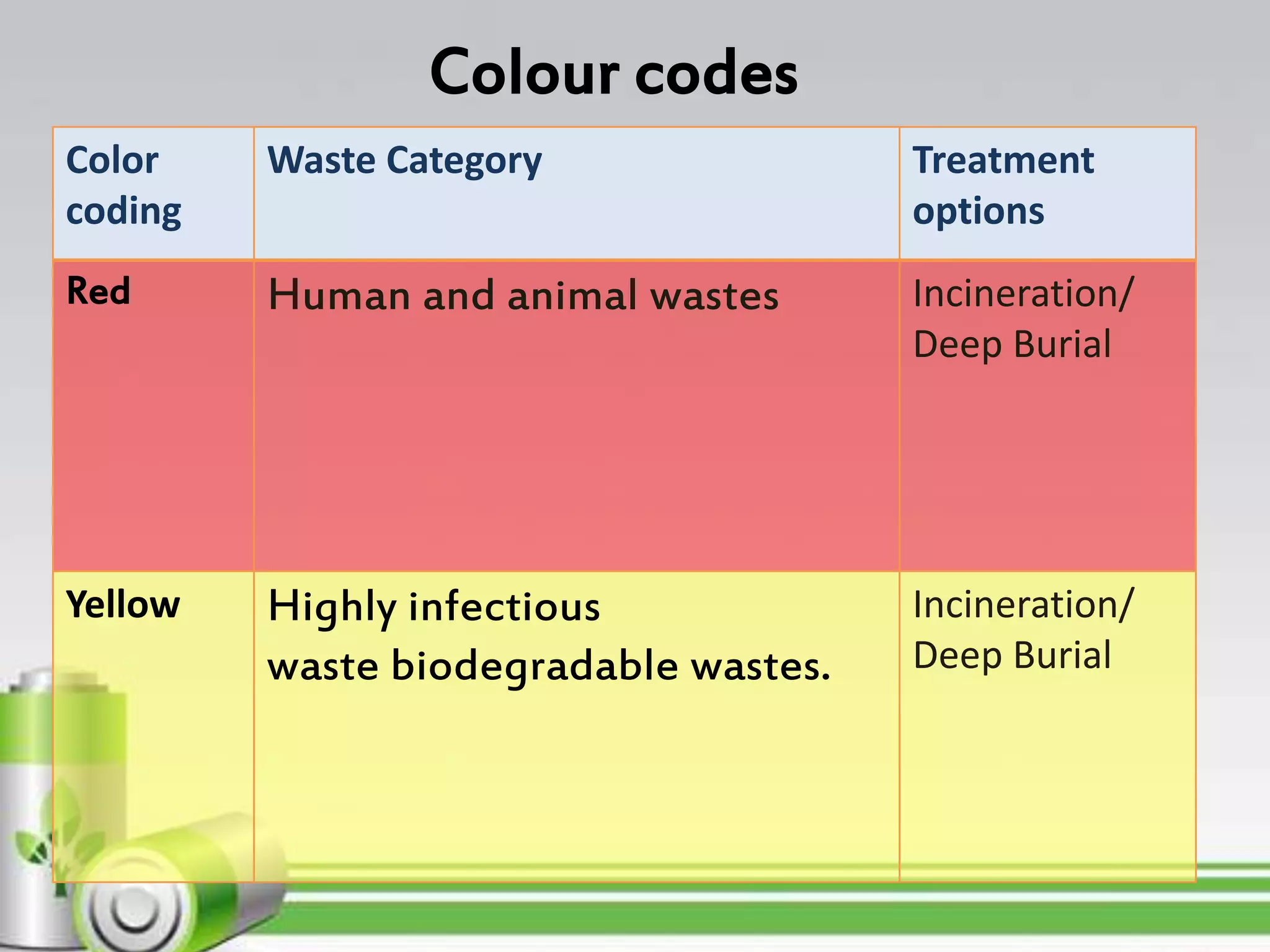
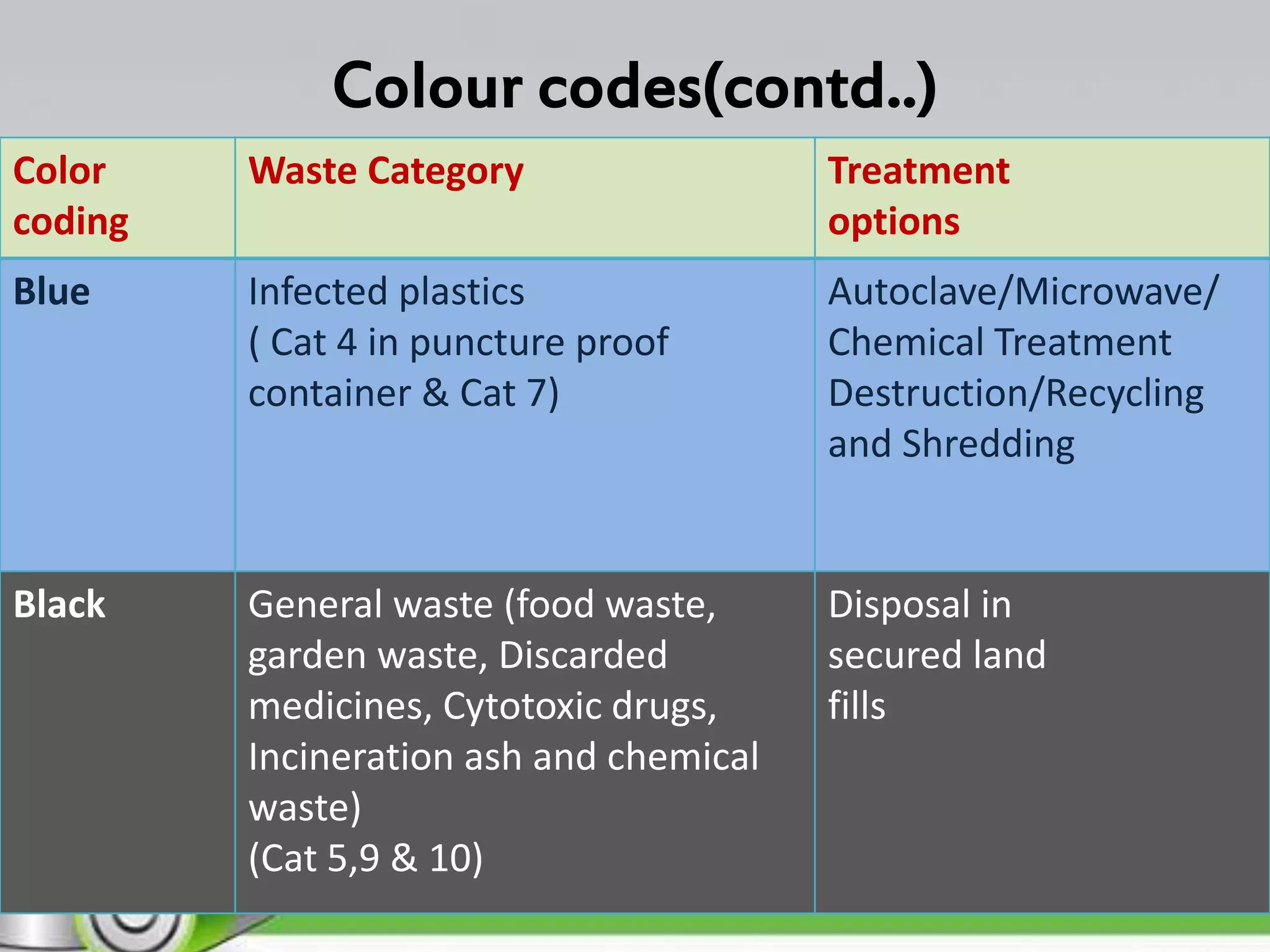
Standard precautions are a set of practices used to prevent the spread of infections in healthcare settings. They include proper hand hygiene, use of personal protective equipment, safe handling of sharps, and appropriate waste disposal. Healthcare facilities must properly segregate, disinfect or sterilize, and dispose of biomedical waste to prevent the spread of infections. Waste is categorized and disposed of according to color-coded bags through methods like incineration, autoclaving, or deep burial. Proper waste management and staff training are essential to reduce the risks posed by biomedical waste.























































![BMW[1].pptx community health nursing-2..](https://cdn.slidesharecdn.com/ss_thumbnails/bmw1-240521182705-3424b4e1-thumbnail.jpg?width=640&height=640&fit=bounds)


















































































