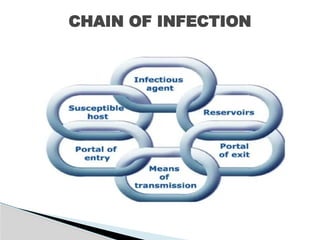
The document addresses infection prevention and control, defining various infectious agents and their environments, and the importance of healthcare-associated infections. It outlines standard safety measures, bio-medical waste management, and the need for personal protective equipment to mitigate risks for healthcare workers and patients. Furthermore, it emphasizes the role of an infection control committee in the hospital and the management of antibiotics and biomedical waste.