Downloaded 267 times








![Mouth temperature / fluid waxes
so called since they are firm at
room temp. & can flow at mouth
temp.
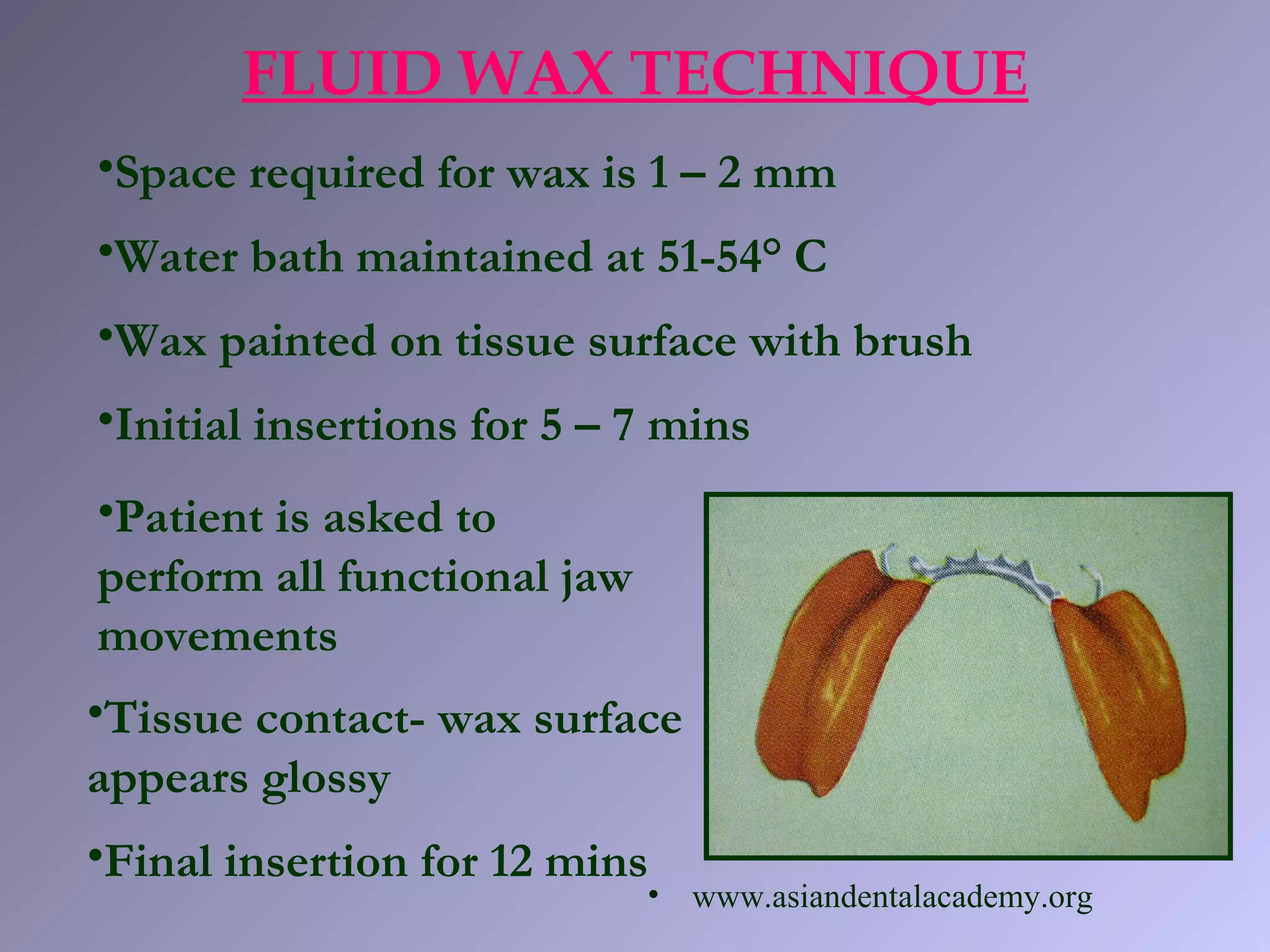
FLUID WAX TECHNIQUE
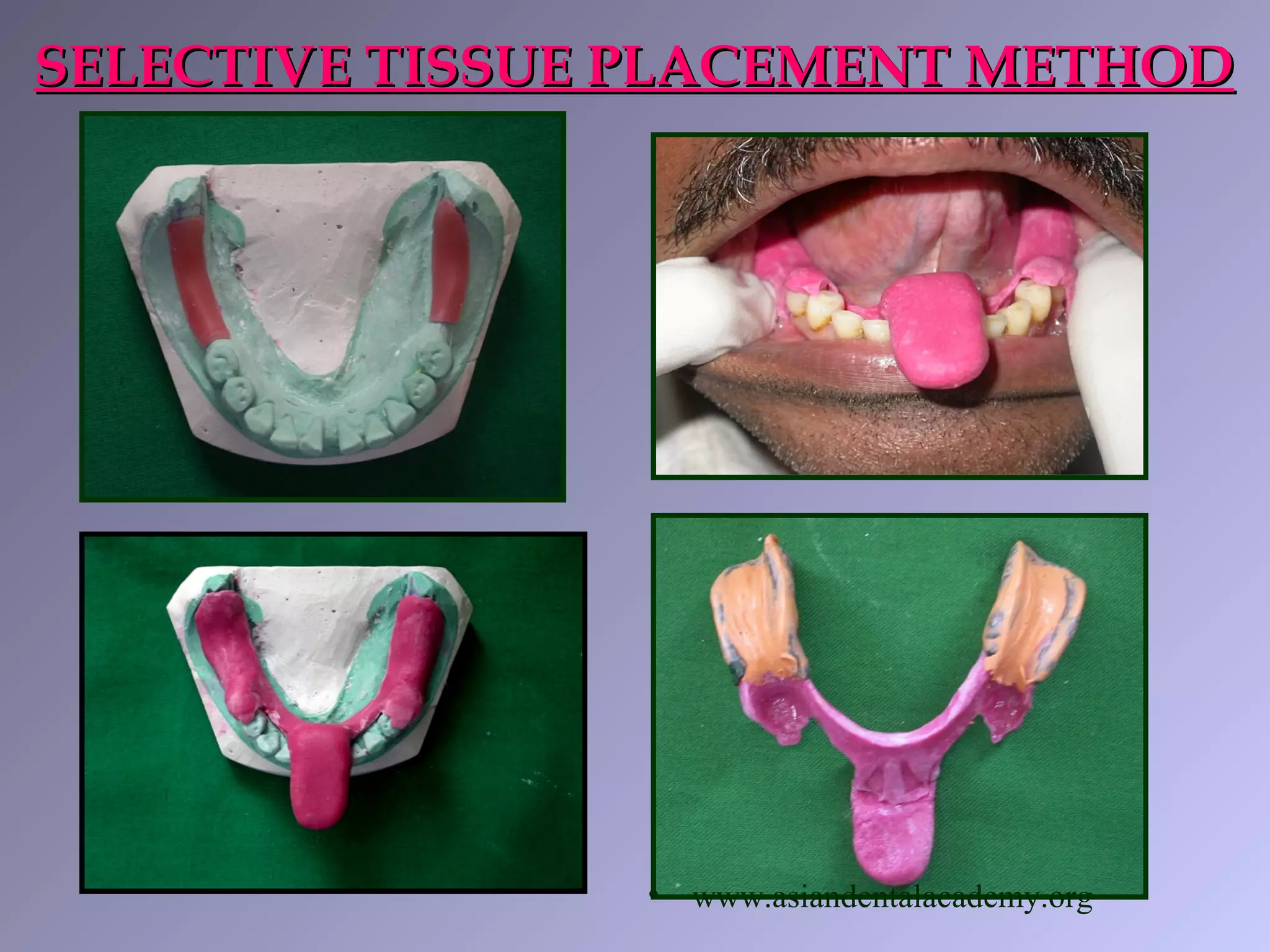
•Korrecta no. IV - tissue surface [orange]
•Korrecta no. I – reinforcement of borders [pink]
By Dr. O.C. Applegate & Dr. S.G.Applegate
• www.asiandentalacademy.org](https://image.slidesharecdn.com/impressiontechniquesinrpd-180720093804/75/Impression-techniques-in-removable-partial-dentures-44-2048.jpg)




This document discusses various impression techniques for removable partial dentures. It describes different types of impression materials and trays used for anatomic and functional impressions. Key techniques discussed include the fluid wax technique, McLean's occlusal loading technique, Hindle's finger loading technique, and Rapuno's single tray dual impression technique. The objectives of a corrective or functional impression are to record tissues under loading and distribute forces evenly. Selective tissue placement aims to direct forces to areas better able to withstand stresses while protecting more vulnerable areas.



















































































