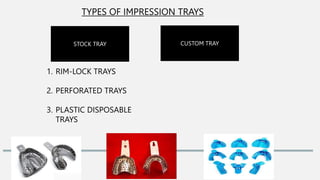
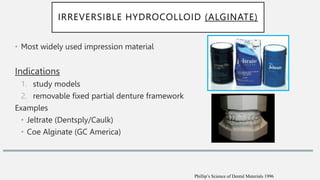
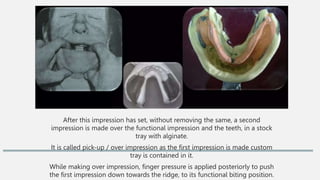
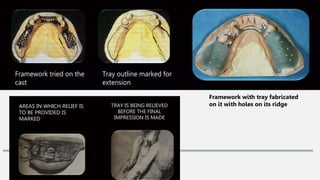
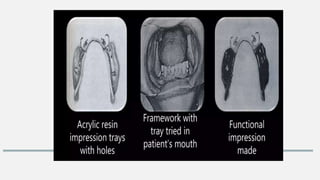
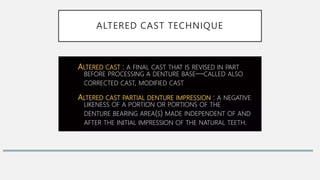
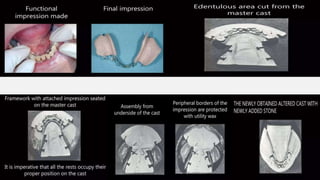
The document outlines impression procedures for removable partial dentures, emphasizing the importance of accurate impressions for proper denture fit. It details various impression techniques, materials, and types of trays, along with their advantages and disadvantages. Additionally, it discusses primary and functional impressions, along with specific methods like selective pressure impressions and the fluid wax technique, concluding that the choice of impression technique is crucial for effective denture fabrication.









































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)