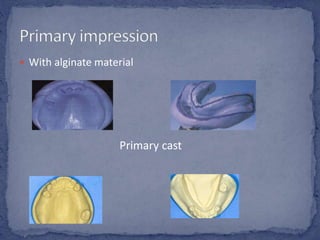
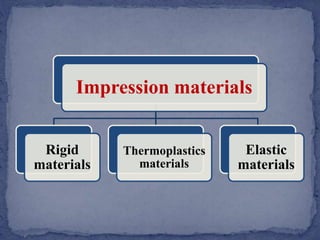
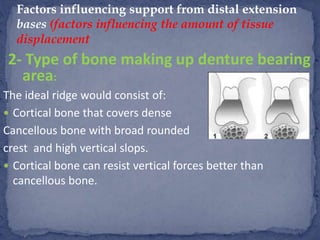
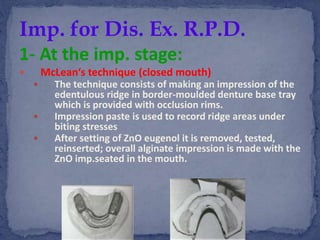
This document discusses various methods and factors related to making impressions for removable partial dentures with distal extensions. It defines different impression materials and techniques, including primary and secondary impressions. Factors that influence support from distal extension bases include the quality of ridges, bone type, denture design, tissue coverage, occlusal forces, anatomy, and fit of the denture base. Techniques discussed for impressions include McLean's, Hindle's, selective tissue placement, and the altered cast method.




























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

