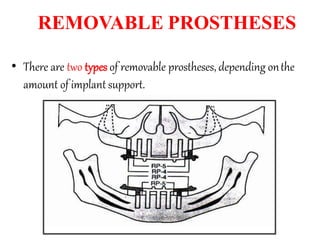
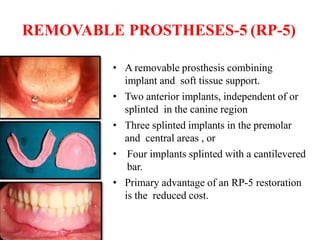
- An implant-supported overdenture is a removable denture that is partially supported by dental implants. It can provide improved function, esthetics, lip support and speech compared to conventional dentures.
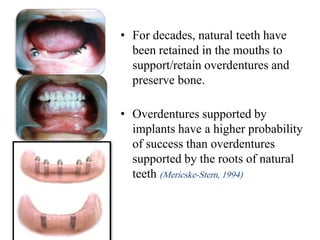
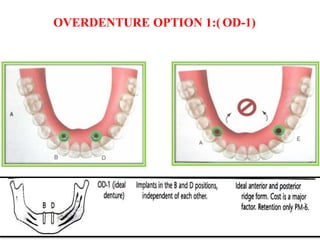
- Overdentures supported by implants have a higher success rate than those supported only by natural tooth roots. A minimum of two implants is recommended to support a mandibular overdenture.
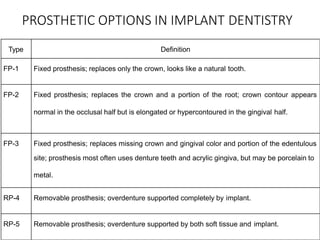
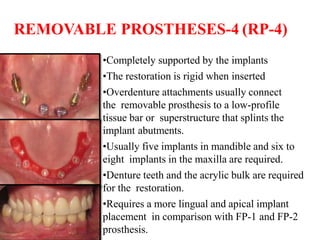
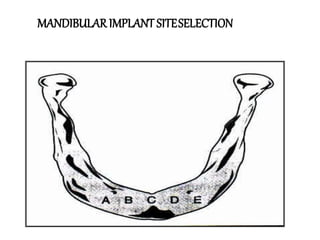
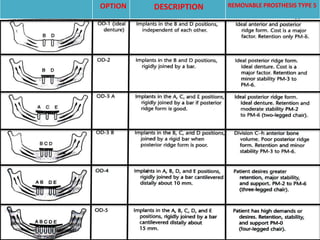
- Treatment planning for implant overdentures involves medical and dental evaluations to determine a patient's suitability and the appropriate type of prosthesis based on their clinical situation.