CONTENTS
Introduction
Definitions
Prosthetic Options
Advantages Of OD
Disadvantages Of OD
Implant OD V/S Fixed
Prosthesis Advantages
Prosthesis Movement
OD Attachments
OD Treatment Options-
Mandible/Maxilla
All On 4 Implants
Review Of Literature
Conclusion
References
DEFINITION
? According toGPT 9:-
Overdenture : Any removable dental prosthesis that covers and rests
on one or more remaining natural teeth, the roots of natural teeth,
and/or dental implants; a dental prosthesis that covers and is
partially supported by natural teeth, natural tooth roots, and/or
dental implants.
? An overdenture is defined as a removable prosthesis
that covers the entire occlusal surface of a root or implant
( Harold W Preiskel)
5.
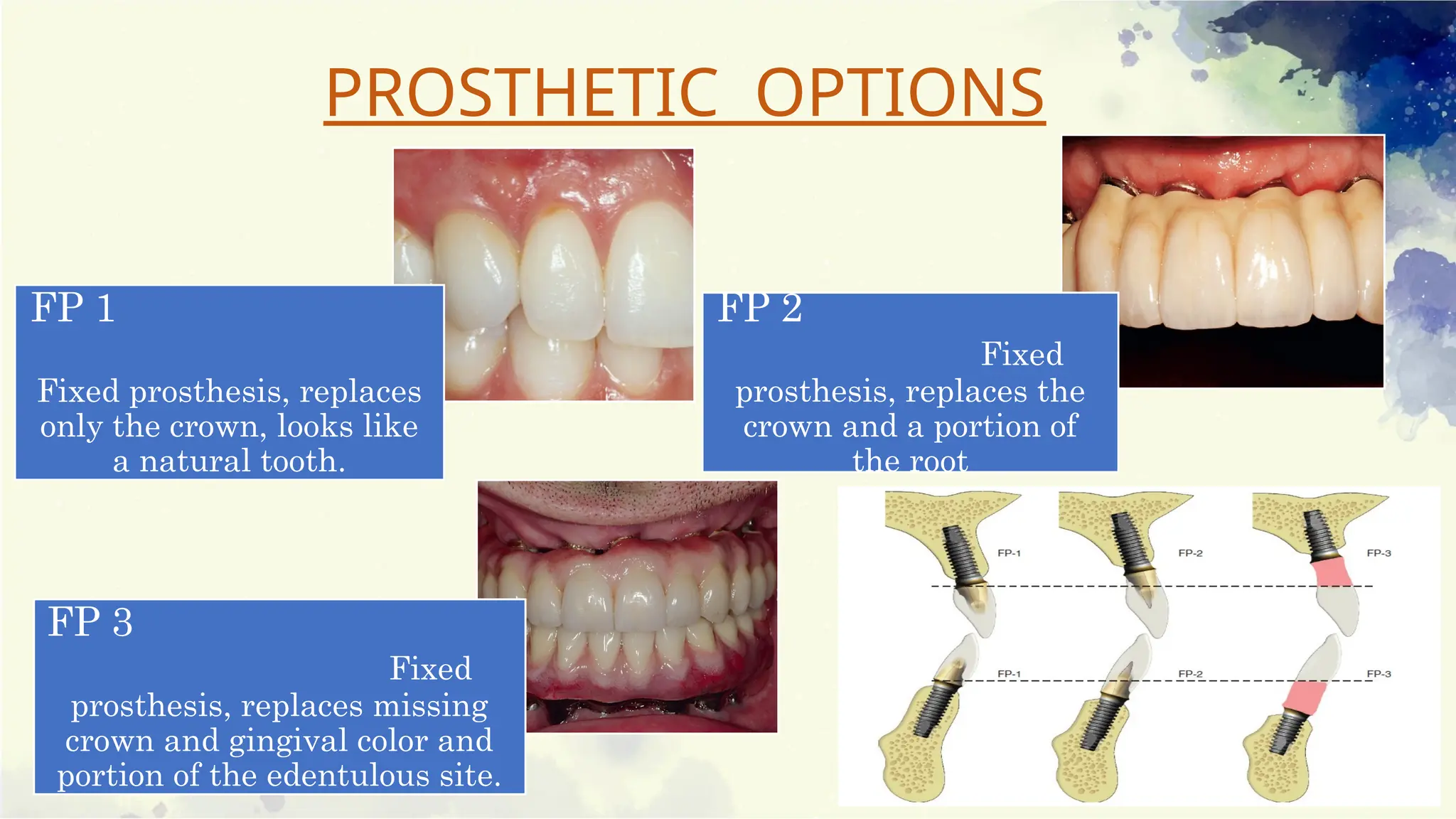
FP 1
Fixed prosthesis,replaces
only the crown, looks like
a natural tooth.
FP 2
Fixed
prosthesis, replaces the
crown and a portion of
the root
FP 3
Fixed
prosthesis, replaces missing
crown and gingival color and
portion of the edentulous site.
PROSTHETIC OPTIONS
6.
RP 4
Removable prosthesis,over
denture supported completely
by implant.
RP 5
Removable prosthesis,
overdenture supported by both
soft tissue and implant
7.
ADVANTAGES OF IMPLANT
SUPPORTEDPROSTHESIS
Minimum/ prevents anterior bone loss
Improved esthetics
Improved stability
Improved occlusion
Decrease in soft tissue abrasions
Improved chewing efficiency and force
Improved retention
Improved support
Improved speech
Reduced prosthesis size
Improved maxillofacial prostheses
8.
DISADVANTAGES OF IMPLANT
SUPPORTEDPROSTHESIS
psychological
Greater abutment crown height space is required.
Long term maintenance
Continued posterior bone loss
Food impaction
Movement (RP-5)
10.
CLASSIFICATION OF
PROSTHESIS MOVEMENT(Misch 1985)
PM0 No movement of prosthesis, requires implant support similar
to fixed prosthesis
PM2 Prosthesis with hinge motion
PM3 Prosthesis with hinge and apical motion
PM4 Allows movement in four directions
PM6 All ranges of prosthesis movement
OVERDENTURE OPTION 1
PatientSelection Criteria
• Opposing a maxillary full denture
• Anatomical conditions are good to excellent
• Posterior ridge form is an inverted U shape.
• Patient’s needs and desires are minimal
• Edentulous ridge, with a tapered dentate arch form
• Cost is the primary factor.
• Additional implants will be inserted within 3 years.
ADVANTAGES
Reduced cost.
Hygiene procedures also are facilitated
DISADVANTAGES
Relatively poor implant support and stability
Future bone loss is not reduced
Increase in prosthetic maintenance appointments
Wear of attachments
18.
OVERDENTURE OPTION 2
PATIENTSELECTION CRITERIA
Opposing arch is a maxillary denture.
Anatomical conditions are good to excellent
Posterior ridge forms an inverted U shape.
Patient’s need and desires are minimal
Patient can afford new prosthesis and connecting bar.
Additional implants will not be inserted for more than 3 years.
Low patient force factors (e.g., parafunction)
OVERDENTURE OPTION 3
PATIENTSELECTION CRITERIA
Opposing arch is a maxillary denture
Anatomical conditions moderate to
excellent
Posterior ridge forms inverted U shape
Patient’s needs and desires require
improved retention, support, and
stability
Cost a moderate factor
Patient may have moderate force factors
23.
Advantages of SplintedA, C, and E Implants
Six times less bar flexure compared with A and E positions
Less screw loosening
Less metal flexure
Three implant abutments
Less stress to each implant compared with A and E implants
Greater surface area
More implants
Greater anteroposterior distance
24.
OVERDENTURE OPTION 4
Four implants are placed in the A, B, D, and E positions.
Patient has opposing maxillary teeth or c–h anterior
bone volume with CHS greater than 15 mm.
Distal cantilever up to 10 mm on each side if the stress
factors are low.
25.
PATIENT SELECTION CRITERIA
Moderate to severe problems with traditional dentures
Needs or desires are demanding
Need to decrease bulk of prosthesis
Inability to wear traditional prostheses
Desire to abate posterior bone loss
Unfavourable anatomy for complete dentures
Problems with function and stability
Posterior sore spots
Opposing natural teeth
C–h bone volume
Unfavourable force
26.
OVERDENTURE OPTION 5
Five implants are inserted in the A, B, C, D, and E positions.
The superstructure is usually cantilevered distally up to two times
the A-P spread and averages 15 mm, which places it under the
first molar area
27.
PATIENT SELECTION CRITERIA
Moderate to severe problems with
traditional dentures
Needs or desires are demanding
Need to decrease bulk of
prosthesis
Inability to wear traditional
prostheses
Desire to abate posterior bone loss
Unfavorable anatomy for
complete dentures
Problems with function and
stability
Posterior sore spots
Moderate to poor posterior
anatomy
Lack of retention and stability
Soft tissue abrasion
Speech difficulties
More demanding patient type
29.
MAXILLARY OVERDENTURE
Onlytwo treatment options are available.
Independent implants are not an option because bone quality and
force direction are severely compromised.
Cantilever bars are usually not recommended
The crown height space:
15 mm-anterior space
12 mm- posterior space
30.
ADVANTAGES OF RP4MAX OD
Ability to provide a flange for maxillary lip support
The improved sulcular hygiene
Reduced laboratory fee
31.
TREATMENT OPTIONS
RP-5 prosthesis:four to six implants in three to five arch positions
RP-4 prosthesis: six to 10 implants in all five arch positions
32.
OPTION 1: MAXILLARYRP-5 IMPLANT
OVERDENTURE
Four to six implants supporting a RP-5
prosthesis, of which three are usually
positioned in the premaxilla.
Implants should be at least 9 mm in length
and 3.5 mm in body diameter.
33.
Six implantsare often indicated for a RP-5 prosthesis when force
factors are greater.
The implants are always splinted together with a rigid bar.
34.
Advantages
Retention andstability from the implants.
Posterior support is obtained from the soft tissue.
Maintenance of the premaxillary bone because of the implant
stimulation.
35.
OPTION 2: MAXILLARYRP-4 IMPLANT
OD
6 to 10 implants, which is rigid during
function.
Bilateral canines and distal half of the first
molar positions
Additional posterior implants are located
bilaterally in the pre- molar position,
preferably the second premolar site.
In addition, at least one anterior implant
between the canines often is the anterior
implant often may be placed in the incisive
canal.
36.
The sixto 10 implants are splinted together around the arch with
a rigid bar.
Four or more attachments are usually positioned around the arch.
37.
ALL ON 4IMPLANTS (Paulo Malo)
Allows the rehabilitation of edentulous jaws
without bone graft in one surgical step
through the placement of four implants,
optimizing the available bone.
38.
Advantages
No anatomicalstructures interference.
Angled implant reduces cantilevering.
Immediately provisional bridge can be fabricated
Teeth in a day
No ill fitting dentures any more
Feel and function just like natural teeth
39.
Disadvantages
Free handarbitrary surgical placement of implant is not always
possible
Length of cantilever in the prosthesis cannot be extended beyond
the limit.
It is very technique sensitive and requires elaborate pre-surgical
preparation
40.
ALL ON 6DENTAL IMPLANTS
The standard of care for full arch rehabilitation with dental
implants when the quality and the quantity of the alveolar jaw
bone is excellent.
41.
ATTACHMENTS USED TORETAIN
OVERDENTURE (Since 1960s)
Pillars of implant supported OD.
42.
According to retentivemeans
Frictional
Mechanical
combination
Magnetic attachments
Attachments based on resiliency
Rigid non resilient attachment
Restricted vertical resilient attachment
Hinge resilient attachment
Combination resilient attachment
Rotary resilient attachment
Universal resilient attachment
43.
Stud attachments
Resilient
Non resilient
Ball attachments
O- ring, ERA system & Spheroflex
Bars
Dolder & Hader
Locator attachment system
Zaag attachment system
OT equator
Hybrid bar system
44.
O - RINGATTACHMENT SYSTEM
Elastomeric retentive attachments
Doughnut shaped
Consisting of a ball and a socket
The O-ringpost usually is made of machined titanium alloy.
The post has a head, neck, and body.
The head is wider than the neck and the O-ring is compressed
over the head during insertion.
Typically three sizes of O-rings are used in implant prostheses.
47.
ADVANTAGES
Simplicity indesign
Good retention
Ease of use and maintenance
Low cost
Varying degrees of retention
Possible elimination of a
superstructure.
48.
ERA SYSTEM
Resilientprecision OD attachment.
Universal hinge with vertical movement
4 color codes
Types (based on interocclusal distance)
Standard
Micro
49.
LOCATOR ATTACHMENT
Zestanchors, escondido, CA, USA) in 2001.
Classified as universal hinge.
Dual retention
50.
O T EQUATOR
Rhein83 . The newest line of low profile castable and
direct implant overdenture attachments.
Low vertical profile - 2.1 mm and diameter of 4.4 mm
Can be used when vertical space limitations are a consideration.
51.
BAR AND CLIPTYPE
ATTACHMENTS
Bar joint (resilient)
Single sleeve
Multiple sleeves
Bar unit (non-resilient).
Provides good retention and stability.
52.
DISDVANTAGES
Vertical dislodgement
Fabrication is technique sensitive
Higher cost
Maintenance of hygiene is difficult
Frequent loosening of retentive clips.
53.
HADER BAR ANDCLIP
Helmut Hader (1960s)
Hader EDS system. Donnel, and Staubli in 1992
Three different retention strengths and a 20-degree clip rotation to
improve flexibility.
54.
DOLDER BAR
Theyare classified as combination resilient attachments
Due to its adjustability, it is easy to control the retention provided
by the bar.
55.
MAGNETIC ATTACHMENTS
Madeup of mainly aluminum-nickel-cobalt metals.
Classified as universally resilient attachments
ADVANTAGES
Shorter so can be used in cases of reduced inter-
arch space.
56.
DISADVANTAGES
Streaking- MRI
Least retention
Heating during sterilization leads to decrease in retentive
forces in long-term use.
Get corroded in saliva on long-term use
57.
CONCLUSION
Implant-supported overdenture provesto be a better treatment
alternative to the conventional denture. Hence, this treatment
modality should be practiced whenever indicated. It will preserve
hard and soft tissues of the patient and give psychological relief to
the patient.
10/05/2025 60
TYPE OFIMPLANT ABUTMENT CONNECTION
• The implant-abutment interface determines joint strength, stability,
and lateral and rotational stability.
10/05/2025 64
TWELVE-POINT HEXAGON
•It allows for more options for abutment placement over
the fixture.
• Allows placing the abutment on implant for every 30°
angulation
THREE-POINT INTERNAL TRIPOD
• Triangular internal geometry with trichannel design.
• Disadvantage of this design is that it allows for
positioning of the abutment on fixture only at every
120°
65.
10/05/2025 65
INTERNAL OCTAGON
•Eight-sided internal geometry and allows for positioning of abutment at
every 45°.
• Offers minimal rotational and lateral resistance during the function.
MORSE TAPER
• Tapered projection from implant abutment that fits into a
corresponding tapered recess in the implant.
• Leading to the friction fit and cold welding at the interface.
66.
10/05/2025 66
ABUTMENT MATERIALS
TITANIUM
•Excellent biocompatibility.
• Used for custom made abutments as well as prefabricated
abutments.
ALUMINA
• Alternative to titanium abutment to meet the high esthetic
demands.
• High incidence of fractures
ZIRCONIA
• Denser and significantly stronger than alumina.
• Material of choice for all anterior restorations.
67.
10/05/2025 67
METAL ALLOYS
•Cast restorations that are screw-retained ,used when there is a
limited amount of interocclusal space.
• Not indicated when the implants are short and deeply placed to
avoid peri-implant tissue inflammation.
PEEK
• Indicated as temporary abutments.
10/05/2025 69
PREFABRICATED (STOCK)ABUTMENTS
STANDARD ABUTMENT
• Use is usually limited to multiunit restoration, especially in non-esthetic zones.
• Margin of the abutment remains supragingival.
• It allows easy maintenance and
• Margins can be easily inspected.
70.
10/05/2025 70
CONICAL ABUTMENT
•Commercially known as EsthetiCone.
• Used in esthetic areas for multiple as well as single unit restorations.
• Allows for a good emergence profile.
• Disadvantage: Collar height is uniform circumferentially and it can result in collapse of the
interproximal gingiva.
71.
10/05/2025 71
ANGULATED ABUTMENT
•Allows for correction of angulation and positional discrepancy.
• Available in 15 to 35° angulations.
• The implant surface of the angulated abutment is 12-sided internally; this shape allows it
to fit onto the hexed implant in 12 different ways to simplify the abutment positioning.
72.
10/05/2025 72
CEMENTABLE CORE
•Commercially, it is known as CeraOne system.
• The prosthesis which is cemented onto the abutment is fabricated on a core made of either a
gold alloy or a ceramic material.
• Indicated, especially for single tooth replacements.
73.
10/05/2025 73
POST ABUTMENT
•It is screwed onto an implant intraorally or on implant analog in a master cast and prepared
similarly like a tooth in fixed prosthodontics.
74.
10/05/2025 74
BALL ABUTMENT
•It is a prefabricated abutment used for the retention of a
tissue-supported overdenture.
• It is available in multiple heights for varying tissue collar.
• Ball abutments can be used with either O-ring attachments or
nylon inserts.
10/05/2025 77
CUSTOM ABUTMENT
•Allow for an individual emergence profile of the reconstruction directly by the abutment.
• Fabricated by either copy-milling techniques or CAD/CAM systems
78.
10/05/2025 78
ABUTMENT SELECTIONCRITERIA
IMPLANT POSITION
ANGULATION OF IMPLANT
INTER OCCLUSAL SPACE
TISSUE HEIGHT/ SULCULAR DEPTH
79.
10/05/2025 79
IMPLANT POSITION
•Evaluated as the implant relates to the final prosthesis and the adjacent teeth.
• If the implant lies outside the mesiodistal and buccolingual boundaries of the planned restoration,
then the implant may not be restorable.
80.
10/05/2025 80
ANGULATION OFIMPLANT
• An angulation discrepancy greater than 15 degrees usually requires an
• angulated,
• cementable, or
• custom abutment.
81.
10/05/2025 81
INTER OCCLUSALSPACE
• Corresponds to the vertical distance between the superior surface of the implant and the
opposing dentition in maximum intercuspation.
• Minimum of 2.8 mm of interocclusal space is necessary to restore an implant.
82.
10/05/2025 82
TISSUE HEIGHT/SULCULAR DEPTH
• Distance from the superior surface of the implant to the gingival
margin.
• This is measured 6 to 8 weeks following stage 2 surgery.
• Ideally, in esthetically important areas the margin of the restoration
is 1 to 2 mm subgingival.
• The tissue height is not as critical if the restoration is not in the
esthetic zone and a supragingival margin is planned.
10/05/2025 84
• Theprocess of selecting an abutment involves evaluating the position, angulation, interocclusal
space, and tissue height of a given implant.
• The order of evaluation is extremely important in this method of selection.
• The position is the first consideration.
• The angulation must be evaluated next.
< 15 degree : any abutment other than angulated abutment
15- 35 degree : angulated or custom abutment
>35 degree: custom abutment/ non restorable
85.
10/05/2025 85
• Interocclusalspace
<2.8 mm : non restorable
2.8 mm : cylindric abutment
3.5 mm : cylindric/ post abutment
4.5 mm : all abutments except standard, angulated& cementable core
5.0 mm : all except angulated and cementable core
6.0 mm : all except angulated
>7.0 mm : all abutments
86.
10/05/2025 86
Tissue height
<1mm: cylindrical,post, custom made
1- 2mm : all except standard / angulated
2-3mm : all abutments
3-5mm : all except cylindrical
>5mm : all except cylindrical / post
10/05/2025 88
CONCLUSION
• Tomeet the demand for improved abutments, the implant industry developed an
overwhelming number of components. As a result, selecting an abutment has
become overly complex and confusing.
• The decision on the choice of abutment is based on many factors of which the
clinical situation and clinician’s personal preference leads the selection procedure.
89.
REFERENCES
Misch,_carl_e._Dental_implant_prosthetics
PrasadD K, Prasad D A, Buch M. Selection Of Attachment Systems In Fabricating An
Implant Supported Overdenture. J Dent Implant 2014;4:176-81.
Mukherjee S, Banerjee S, Chatterjeed, Deb S, Swamy Sn, Mukherjee A. All-on-four
Concept In Dental Implants. Int J Oral Care Res 2018;6(2):s77-79
All On 4 The Basics. Anandh Et Al.Biomed. & Pharmacol. J., Vol. 8(spl. Edn.), 609-612
Circumferential Bone Loss Around Splinted And Non-splinted Immediately Loaded
Implants Retaining Mandibular Overdentures: A Randomized Controlled Clinical Trial
Using Cbct. Elsyad Ma Khirallah As. J Prosthest Dent 2016;116(5):741-8 104
A Functional Impression Technique For An Implant-supported Overdenture: A Clinical
Report Uludağ B1, Sahin V. J Oral Implantol. 2006;32(1):41-3.
90.
1. Kucey BKS,Fraser DC. The Procera abutment—The fifth generation abutment for dental implants. J Can
Dent Assoc 2000 Sep;66(8):445-449
2. Rudi C, Guan H, Chaye LY, Newell WJ. Comparative analysis of internal and external-hex crown connection
systems—a finite element study. J Biomed Sci Eng 2008;1:10-14.
3. Abichandani SJ, Nadiger R, Kavlekar AS. Abutment selection, designing, and its influence on the
emergence profile: A comprehensive review. Eur J Prosthodont 2013;1:1-10
4. Karunagaran S, Paprocki GJ, Wicks R, Markose S. A review of implant abutments--abutment classification
to aid prosthetic selection. The Journal of the Tennessee Dental Association. 2013 Fall-Winter;93(2):18-
23; quiz 23-4. PMID: 24611217.
5. Lemos CAA, Verri FR, Bonfante EA, Santiago Júnior JF, Pellizzer EP. Comparison of external and internal
implant-abutment connections for implant supported prostheses. A systematic review and meta-analysis.
J Dent. 2018 Mar;70:14-22. doi: 10.1016/j.jdent.2017.12.001. Epub 2017 Dec 6. PMID: 29221955.
6. Lemos CAA, Verri FR, Bonfante EA, Santiago Júnior JF, Pellizzer EP. Comparison of external and internal
implant-abutment connections for implant supported prostheses. A systematic review and meta-analysis.
J Dent. 2018 Mar;70:14-22. doi: 10.1016/j.jdent.2017.12.001. Epub 2017 Dec 6. PMID: 29221955.
Editor's Notes
#3 Treatment with conventional complete denture is successful when residual alveolar ridges are favorable.
But such treatment will not be successful when,
Residual alveolar ridges are resorbed
Movement of denture leads to discomfort, pain, poor function.
The patients with poor neuromuscular control.
These difficulties can be overcome by the use of osseointegrated implants to support,
retain and stabilize dentures.
#15 2 implants – B and D positions
The implants remain independent of each other and are not connected with a superstructure.
The most common type of attachment used – O-ring or Locator design.
The IOD must be RP-5
#16 The implants should be perpendicular to the occlusal plane.
The hinge rotation should be at 90 degrees to the rotation path.
The two independent implants should be positioned at the same occlusal height.
The implants should be equal distance off the midline.
#19 The implants are positioned in locations B and D
But they are splinted together with a superstructure bar without any distal cantilever
The ideal distance between the implants is in the 14 to 16mm range
#20 Implants are joined with anterior curved bar.
Greater bar flexibility (nine times the B and D positions)
Increased screw loosening
Increased moment forces on anterior aspect of prosthesis
Implants joined with straight bar are lingual to ridge.
Difficulty with speech
Anterior tipping of overdenture
Five times greater bar flexure than B and D positions
Bite force is higher than for B and D positions.
Greater lateral load from prosthesis to implants.
#22 Three root form implants are placed in the A, C, and E positions
A superstructure bar connects the implants but with no distal cantilever
#23 One-half moment force compared with A and E implants
Less prosthesis movement
One implant failure still provides adequate abutment support
#30 If the maxillary lip requires additional support, two options are available:
A bone or soft tissue graft to the premaxilla is performed before or in conjunction with implant insertion or at uncovery for a fixed implant prosthesis.
A maxillary IOD is fabricated with a labial flange on the prosthesis.
#32 Implant positions- bilateral canine regions and at least one central incisor position.
Other secondary implants -first or second premolar region.
#33 No distal cantilever, and the bar design should follow the dental arch form.
The prosthesis should have at least two directions of movement.
A Dolder clip or O-ringThe maxillary RP-5 IOD is designed exactly as a complete denture with fully extended palate and flanges.
#35
In addition, at least one anterior implant between the canines often is the anterior implant often may be placed in the incisive canal.
#36 Palatal coverage is maintained.
Occlusal scheme – centric occlusion around the arch and only anterior contact during mandibular excursions
#37 The four implants are placed: two posteriorly tilted between 30° and 45° and two anteriorly axial, well anchorated achieving a primary stability of at least 30Ncm.
Indicated with a minimum bone width of 5mm and minimum bone height of 10mm from canine to canine in maxilla and 8mm in mandible
#40 By placing 6 implants in each jaw, molar to molar rehabilitation is possible giving a minimum of 12 crowns.
#41 To enhance the retention, the stability and support of overdentures together with the implants, increases longevity.
An overdenture attachment permits movement during function and removal from the mouth.
The attachment should offer the possibility of controlling the degree of retention.
#44 Has the ability to bend with resistance and return back to their original shape.
O-ring abutments are available in different designs and sizes, with gingival cuffs of varying lengths.
Placed slightly supragingival, with approximately 1 mm of the cuff protruding above the tissue.
#45 A metal or plastic encapsulator permits the easy replacement of the O-ring after wearing or damage.
This eliminates the need for chairside cold curing of a new attachment in place.
Virtually every O-ring encapsulator has an undercut region that houses the O-ring, called the internal cavity.
The overall size of the encapsulator is larger than the O-ring
#46 O-ring hardness is measured with a durometer.
The resultant numerical rating of hardness ranges from 0 to 100 in a Shore A Scale.
The softest O-rings are usually 30 to 40, and the hardest are 80 to 90.
O ring material - silicone, nitrile, fluorocarbon, and ethylene-propylene.
#47 FAILURE OF O-RINGS
Due to the combined adverse effects of stress and environmental factors
Incorrect o-ring size
Unsatisfactory laboratory technique
Damage during insertion
Poor maintenance.
#49 Advantages
Can be used in cases of limited inter-arch space
Can accommodate inter implant angulations up to 40°.
Disadvantages
They cannot be used in cases where rigid restoration is required
Regular replacement of male nylon part due to constant wear and tear.
#50 Available in two versions, castable and prefabricated titanium abutments
Compatible with any implant system
Manufactured with cuff heights from .5 mm to 7 mm.
Female caps are retained by means of a stainless steel housing ranging in four levels of retention
#51 The ideal length of a single bar should be minimum of 20-22 mm to accommodate two clips.
#53 Round superior aspect and an apron toward the tissue below.
The total height may be as low as 4 mm
Hinge resilient attachment
Provides mechanical snap retention.
#54 It is best-indicated when patient has adequate inter-arch space, and minimum resiliency and maximum retention is required.
#55 They can be used in moderately nonparallel abutments.
Laboratory procedures associated with castings are not necessary.
They are more resilient and allow for free movement of the prosthesis.
#60 antirotational - indicated only in case of multiple units that are splinted together
#62 The goals of new designs are to improve connection stability throughout function and placement and simplify the armamentarium necessary for the clinician to complete the restoration
#63 Most common type of connection that is commercially available.
Abutment can fit over the implant fixture at every 60° angulation thus allowing six different positions.
Proved to distribute forces deep within the implant effectively and, hence, improves the joint stability.
#66 Several alternatives were introduced for the fabrication of
abutments, like gold alloy, stainless steel, nickel chromium
and cobalt chromium alloys
#73 Available in both one and two piece systems.
One piece post, commercially available as cement on crown (COC).
Two piece post as CerAdapt.
The preparation
can be rened intraorally and then a crown is fabricated
which is cemented onto the post.
#74 Black lab use
Yellow extra soft, pink soft, silver standard, violet strong,…metal cap…
#75 Prefabricated abutment available for securing the attachment of an implant-supported overdenture or even a partial denture.
It is available in multiple heights for varying tissue levels along with nylon (male) attachments that are color-coded for variable retention and divergence.
#76 Cylindric abutment allows achieving desired emergence profile by starting restoration at the implant level.
The cylindric abutment is the only implant-level restoration available.
#79 Incorrect positioning > incorrect biologic contours, incorrect location of the access opening, nonaxial loading of the implant.
#80 When using cementable restoration, the angulation is not as critical. since there is no screw-access opening
#81 This interocclusal space is the total height available for the abutment plus the restoration.
#84 . Once it is determined that he implant is in an acceptable position and is restorable, then the clinician can move on to the other 3 evaluation criteria
#87 Dissimilar metal in custom made may cause galvanic current
#88 The overwhelming number of abutments available become more manageable if they are categorized by their properties and furthermore, by evaluating the implant position, angulation, interocclusal space, and tissue height the process of abutment selection can be organized and simplified.
The ultimate goal should be to achieve a harmonious relationship between the soft tissues and the hard tissues, mimicking the natural appearance in color, form, size, texture, and optical properties.