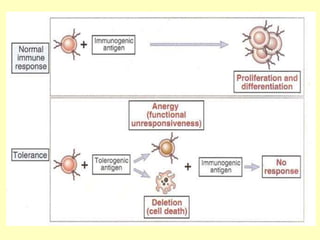
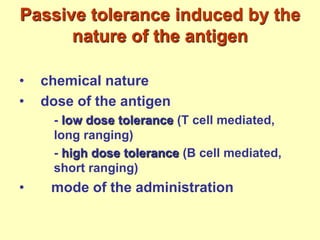
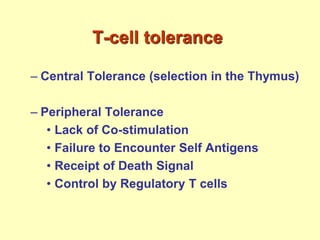
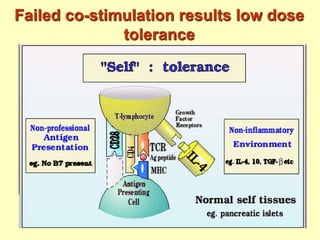
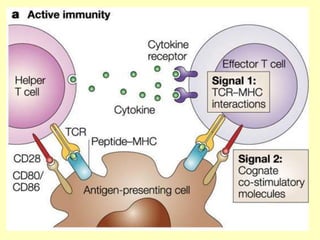
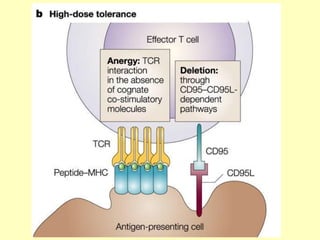
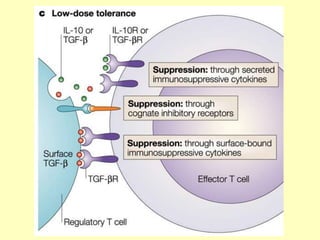
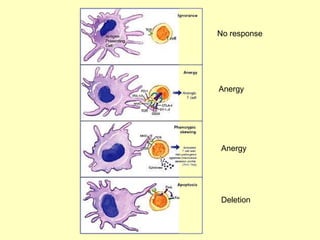
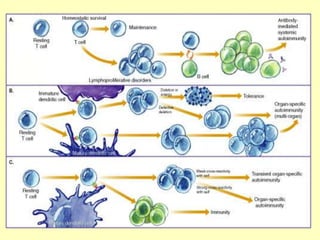
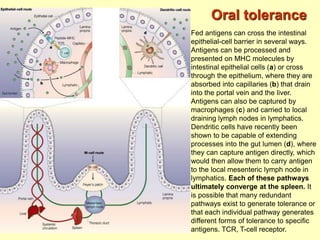
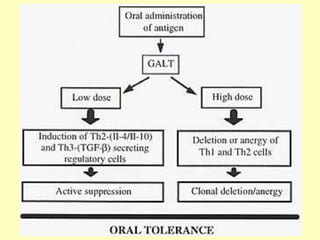
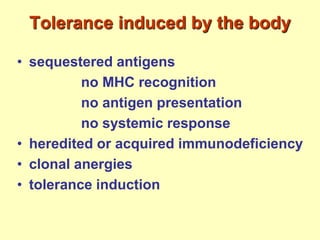
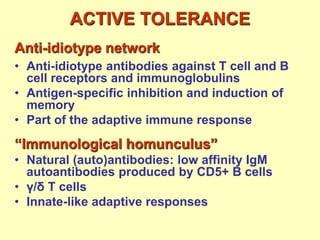
This document discusses immunological tolerance and autoimmune diseases. It explains that the immune system can develop an immune response or enter a state of tolerance upon encountering an antigen. Tolerance is the lack of an immune response to antigens the body has the potential to respond to. Both immune responses and tolerance involve the same cellular and molecular components, differing only in the effector phase. Careful regulation of targeting versus tolerating responses is needed to avoid autoimmunity or failure to respond to pathogens. The document outlines different mechanisms of passive and active tolerance, including central tolerance in the thymus, peripheral tolerance, and oral tolerance through exposure to antigens in the gut.










































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)

![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)











