Download to read offline

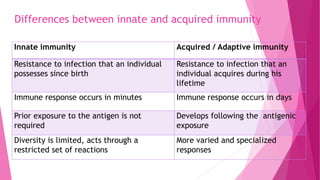
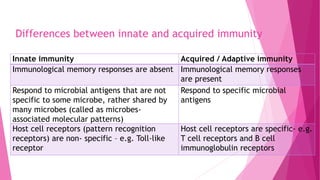
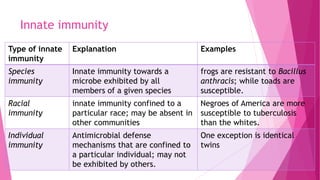
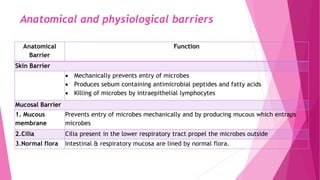
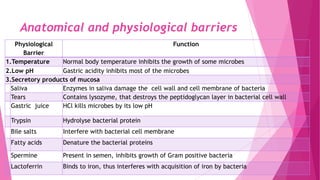
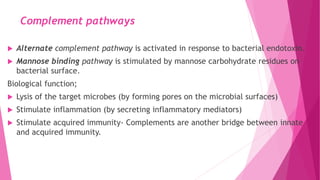

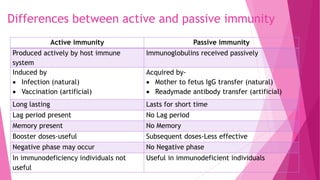


This document defines and compares innate and acquired immunity. Innate immunity is present from birth and provides non-specific resistance to pathogens. It involves anatomical barriers, inflammatory responses, complement pathways, and cytokines. Acquired immunity develops during a person's lifetime through active or passive transfer of antibodies or immune cells. Active immunity results from infection or vaccination and is long-lasting, while passive immunity provides short-term protection through antibody transfer from mother to fetus or through immunoglobulin treatments.

















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















