Downloaded 139 times




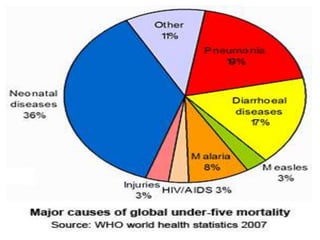









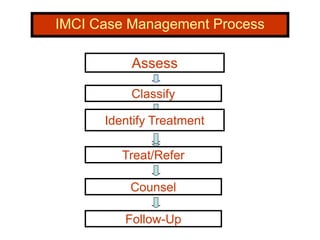
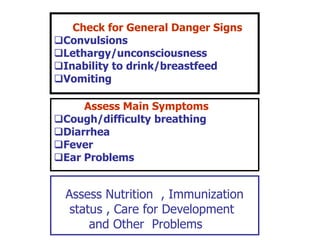
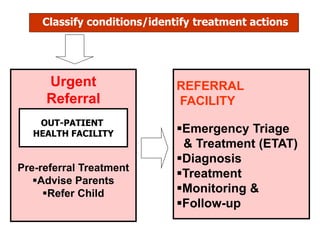
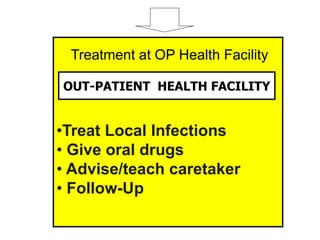
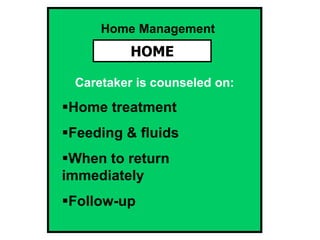
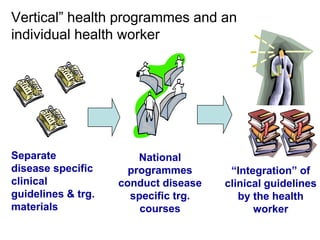



The document discusses Integrated Management of Childhood Illness (IMCI), a strategy developed by WHO and UNICEF to address the major causes of child mortality. IMCI aims to reduce death, illness and disability among children under 5 by improving health workers' ability to assess, classify, treat or refer sick children using syndromic management. It also promotes improved family and community care practices around child health, nutrition and development. The document outlines IMCI's objectives, components and case management process which takes an integrated approach to treating the most common childhood illnesses and ensuring proper nutrition, immunization, counseling and follow-up.










































































































