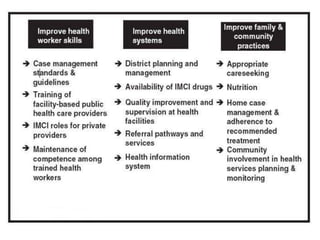
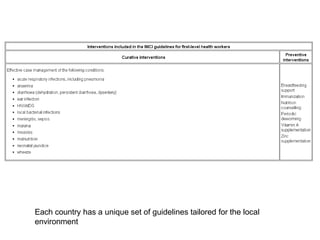
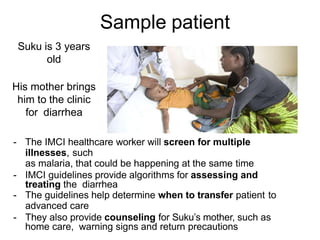
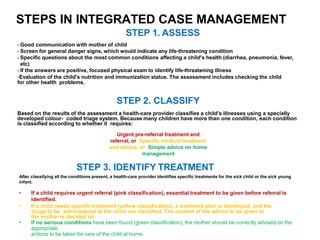
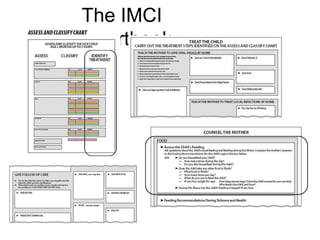
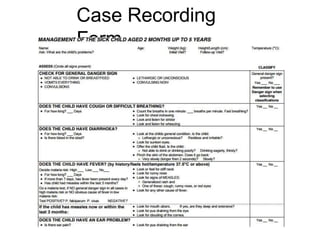
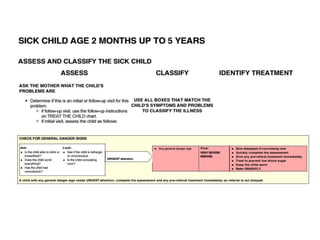
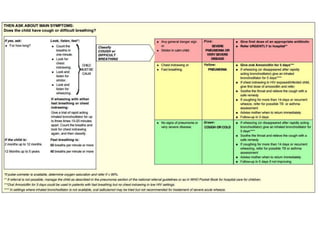
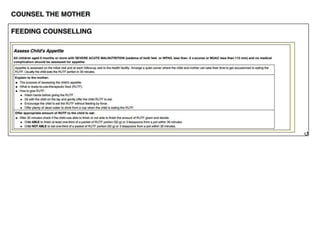
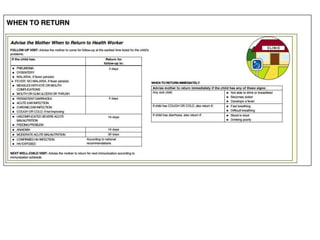
The document summarizes the World Health Organization's Integrated Management of Childhood Illness (IMCI) strategy. IMCI integrates the case management of common childhood illnesses, especially the leading causes of death for children under 5. It provides standardized guidelines and tools for healthcare workers to assess, classify, treat and counsel children with multiple conditions. The goal is to improve the quality of care for sick children and reduce mortality rates through an integrated approach to treating the most common illnesses together.