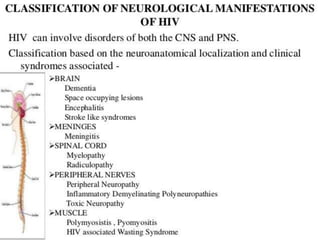
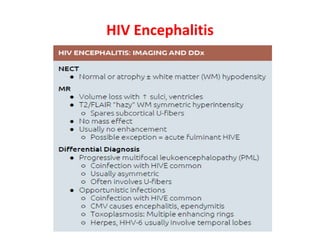
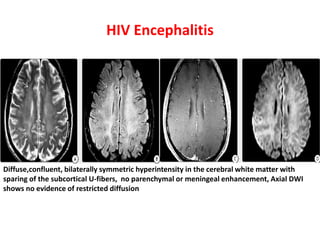
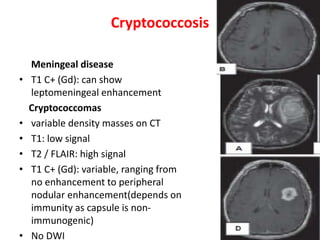
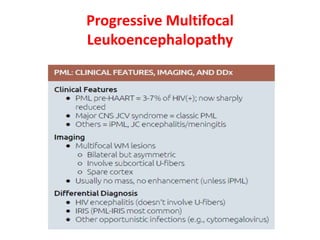
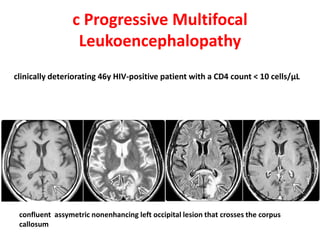
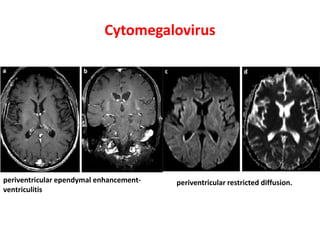
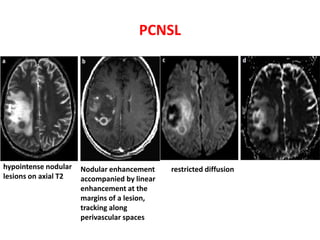
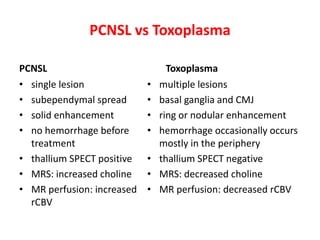
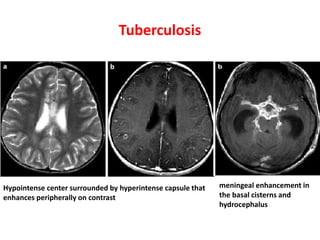
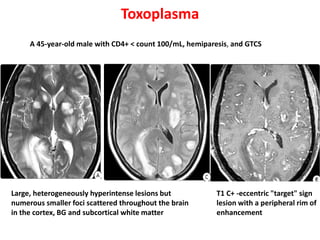
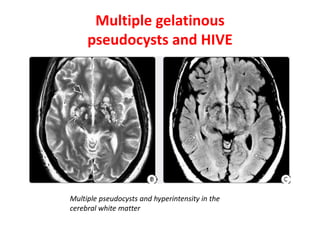
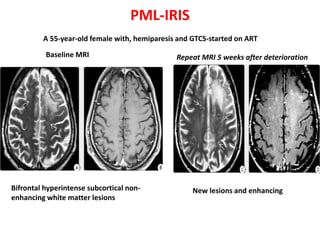
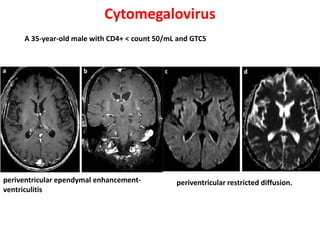
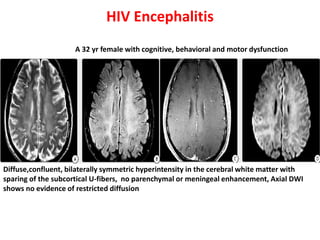
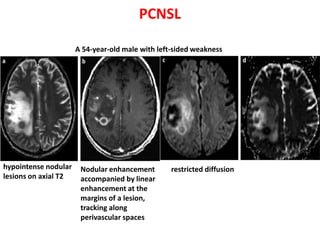
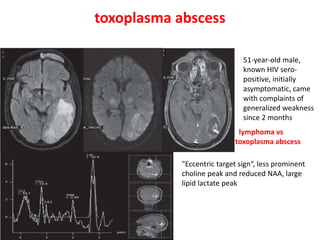
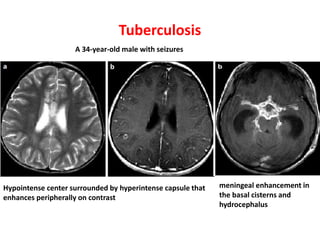
This document discusses the common neurological manifestations seen in patients with HIV/AIDS and their appearance on radiological imaging. It describes HIV encephalitis as the most frequent manifestation, appearing as diffuse symmetric white matter hyperintensities. Toxoplasmosis typically appears as multifocal lesions over 2-3cm with peripheral enhancement. Cryptococcal meningitis can cause leptomeningeal or parenchymal lesions. Progressive multifocal leukoencephalopathy lesions are non-enhancing. Cytomegalovirus commonly involves the periventricular regions. Primary CNS lymphoma often appears as enhancing lesions that cross the corpus callosum. Tuberculosis can cause tuberculomas with peripheral enhancement.
























































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)

































