Downloaded 51 times

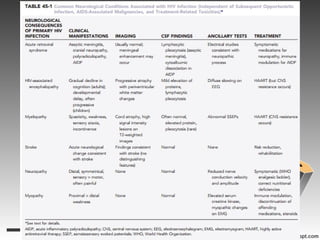
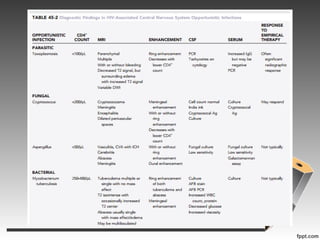
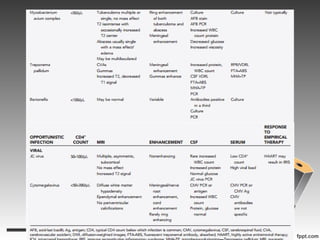


This document summarizes various neurological complications of HIV/AIDS, including: - Acute retroviral syndrome occurring in the majority after initial HIV exposure, potentially causing meningitis. - HIV-associated encephalopathy, the most common HIV-related brain disease, presenting as cognitive and motor slowing. - Myelopathy, characterized by vacuolar changes in the thoracic spinal cord causing spasticity and sensory symptoms. - Several types of infections are described like toxoplasmosis, cryptococcus, CMV, and various types of mycobacteria. - Primary central nervous system lymphoma is an AIDS-defining cancer that can involve the brain, eyes and spinal fluid. - Neurotoxic





































































































