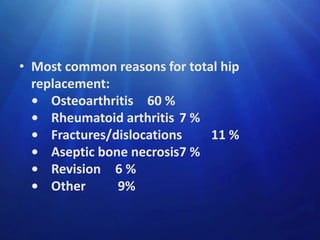
Downloaded 502 times

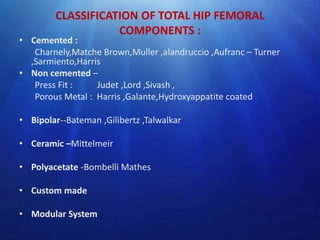


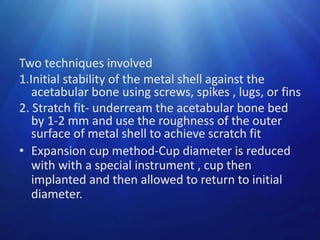
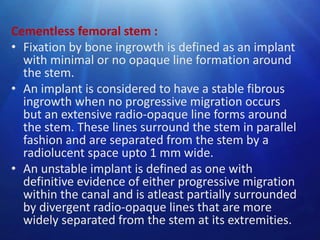
![Metal-on-Metal Bearings
• Metal-on-metal implants seem to be tolerant of
high impact loading, and mechanical failure has
not been reported.
• wear rates less than 10 mm/y for modern metalon-metal articulations
• But there remains major concern regarding the
production of cobalt and chromium metallic
debris, and its elimination from the body.
• metal-on-metal (MOM) bearings have a ‘suctionfit’ less chance of dislocation
(J Bone Joint Surg [Br] 2003;85-B:650-4)](https://image.slidesharecdn.com/hipimplants-dr-140305014058-phpapp01/85/Hip-implants-dr-thahir-51-320.jpg)
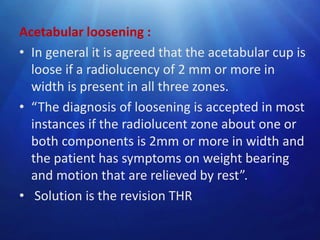
![Ceramic-on-Ceramic Bearings
• Alumina ceramic has many properties that make it
desirable as a bearing surface in hip arthroplasty
• high density- surface finish smoother than metal
implants
• The hydrophilic nature- ceramic promotes lubrication
• Ceramic is harder than metal and more resistant to
scratching from third-body wear particles.
• The linear wear rate of alumina-on-alumina has been
shown to be 4000 times less than cobalt-chrome alloy–
on–polyethylene.
• Ceramic-on-ceramic arthroplasties may be more
sensitive to implant malposition than other bearings. (J
Bone Joint Surg [Br] 2003;85-B:650-4](https://image.slidesharecdn.com/hipimplants-dr-140305014058-phpapp01/85/Hip-implants-dr-thahir-52-320.jpg)






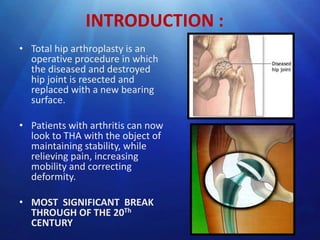
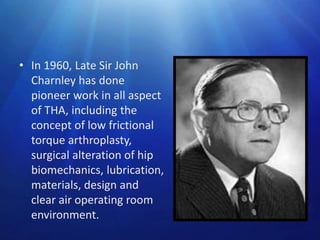
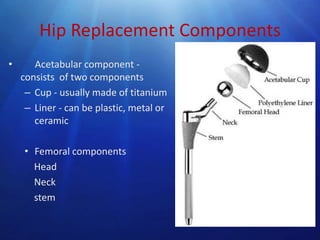
Hip implants are used to replace damaged or diseased hip joints. The document discusses the history and development of hip implants from the 1950s onwards. It describes the key figures like Sir John Charnley who pioneered total hip arthroplasty. The anatomy of the hip joint and biomechanics considerations for implant design are outlined. Different types of femoral and acetabular components including cemented, cementless, and alternative bearing surfaces are explained. Indications, contraindications and risks of hip replacement surgery are also summarized.



































































