Downloaded 29 times

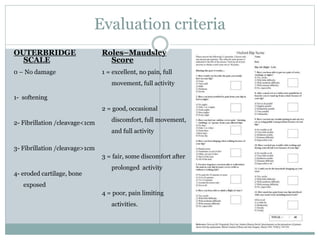

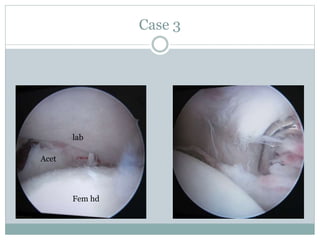
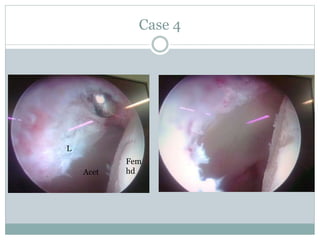
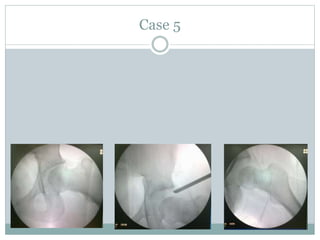
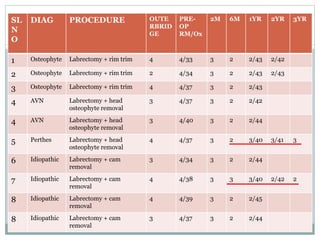

This document discusses femoro-acetabular impingement (FAI), specifically examining the role of labrectomy (labrum removal) in treatment. It presents the case that repairing a damaged labrum may not restore normal hip biomechanics, while labrectomy removes a source of pain and impingement. The author conducted a study of 10 hips that underwent arthroscopic labrectomy for pincer or mixed FAI. Post-operatively, patients showed improved clinical scores up to 2 years follow-up, indicating labrectomy provides short-term pain relief in these cases. However, the study had limitations including a lack of long-term data or comparison to labral repair techniques.










![Femoroacetabular%20 impingement[1]](https://cdn.slidesharecdn.com/ss_thumbnails/femoroacetabular20impingement1-130422051258-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




