Downloaded 13 times

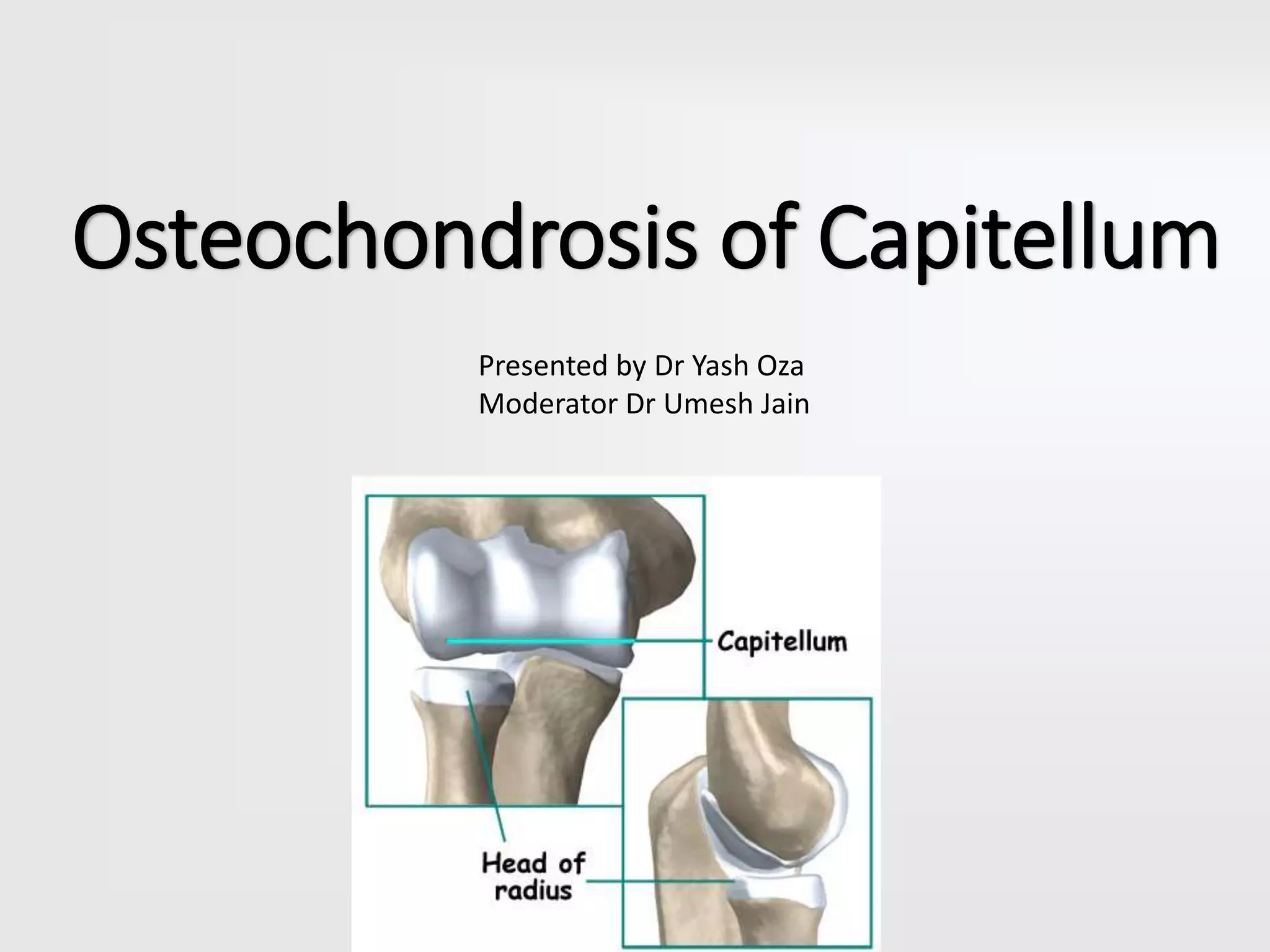
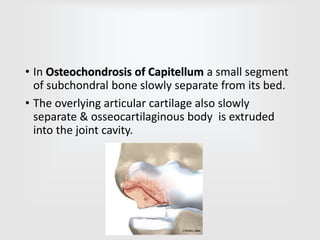
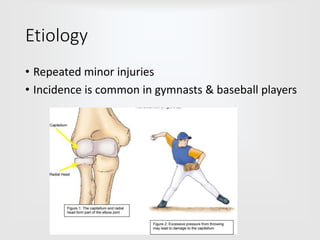
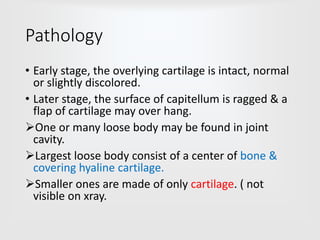
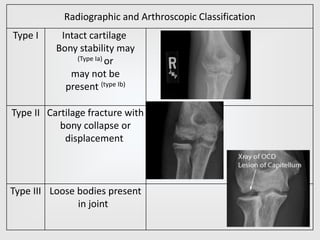
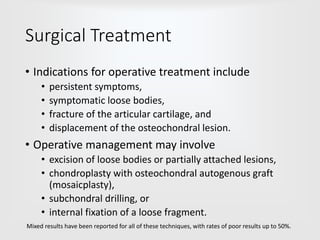
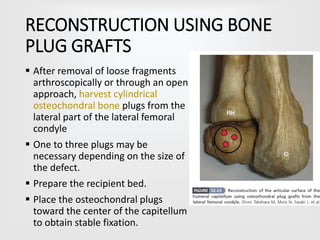

Osteochondrosis of the capitellum is a condition where a segment of subchondral bone and overlying cartilage separate from the elbow. It typically affects adolescent boys and is caused by repeated minor injuries. Early stages show intact or slightly discolored cartilage, while later stages have a ragged capitellum surface and loose bodies in the joint. Treatment involves rest initially, while surgical removal of loose bodies or fragment fixation may be needed for persistent symptoms. Arthroscopic surgery is now preferred over open procedures.








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


