
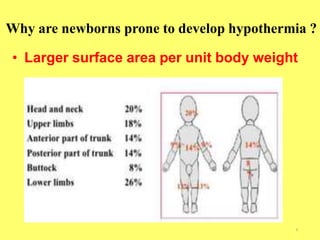
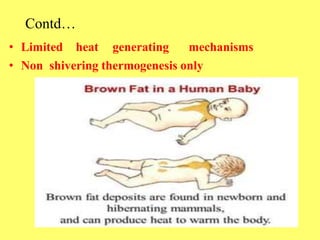
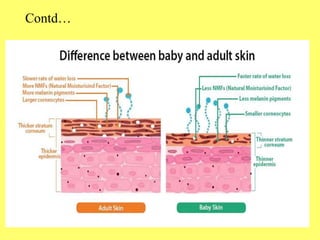
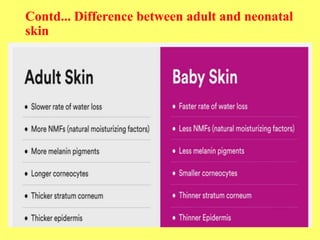
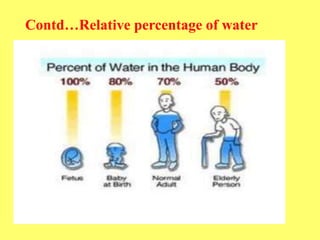
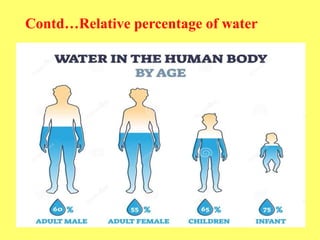
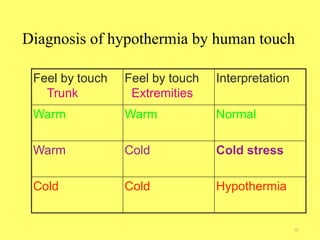
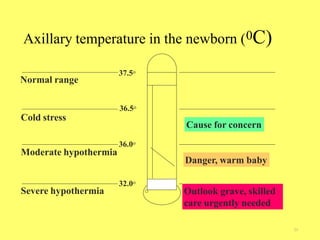
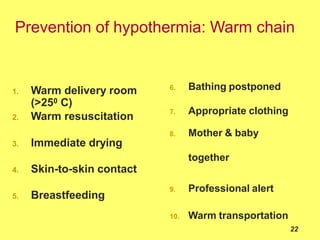
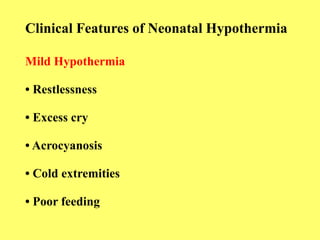
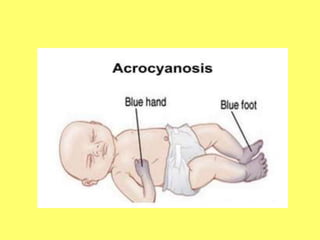


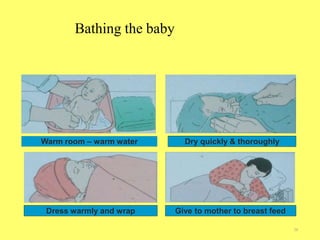



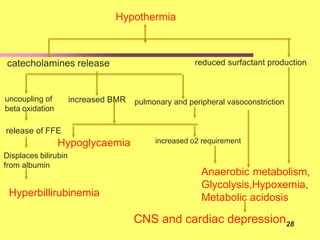









Hypothermia is a significant problem in newborns that can cause morbidity and mortality. It is defined as a body temperature below 36.5°C. Newborns are prone to hypothermia due to their large surface area to weight ratio, limited heat production mechanisms, and inability to thermoregulate well. Hypothermia can be caused by cold environments, wet skin, improper covering, and other situations that increase heat loss or impair heat production. Prevention focuses on keeping newborns warm through skin-to-skin contact, breastfeeding, warming the environment, and delayed bathing. Treatment involves gradual rewarming while monitoring for complications like hypoglycemia and infection.























































































