Download to read offline








![DIAGNOSTIC
EVALUATION
✔ DYSPNOEA
✔ WHEEZING AND COUGHING
✔ ACUTE EXPISODES OF SHORTNESS OF BREATH
✔ HISTORY COLLECTION
✔ PHYSICAL EXAMINATION
✔ PULMONARY FUNCTION TEST
✔ PEAK EXPIRATORY FLOW RATE {PEFR}
✔ BRONCHOPROVOCATION TESTINY
✔ SKIN TESTING
✔ RADIO ALLERGOSORBENT TEST [RAST]
✔ BLOOD COUNT CHEST RADIOGRAPHS](https://image.slidesharecdn.com/pptasthmarespiratory-230710023114-d19829ec/85/PPT_Asthma_Respiratory-pptx-11-320.jpg)






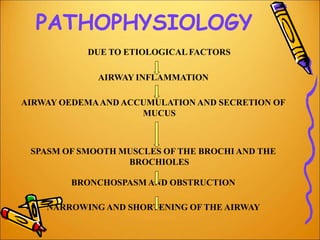
Asthma is a chronic inflammatory disease of the airways characterized by airway hyperresponsiveness and reversible airflow obstruction. It is caused by a combination of genetic and environmental factors such as family history, prenatal sensitization, exposure to allergens and pollutants, and infections. Asthma is classified based on severity from mild to severe. Symptoms include wheezing, coughing, chest tightness, and shortness of breath. Diagnosis involves assessing symptoms and lung function tests. Treatment focuses on bronchodilators and inhaled corticosteroids to prevent symptoms and exacerbations.