Download to read offline

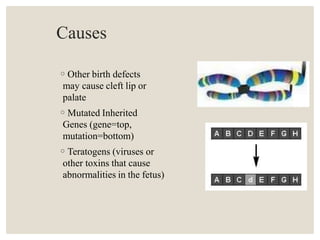
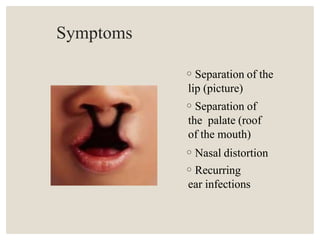
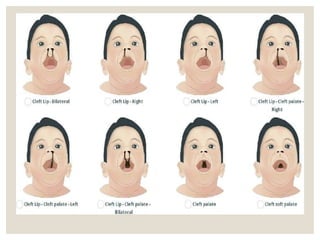
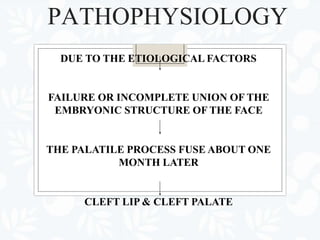
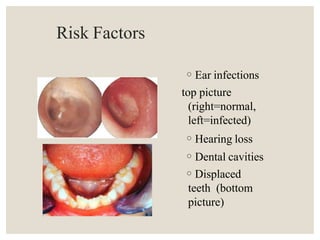
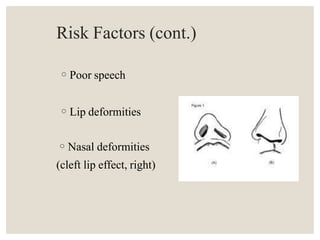
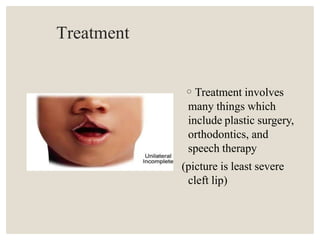







Cleft lip and palate is an abnormal separation of tissues in the oral-facial region that occurs during fetal development. It can be caused by genetic factors, viruses, or other toxins. Symptoms include separation of the lip or palate, nasal distortion, ear infections, feeding difficulties, and speech and dental problems. Treatment involves surgery to repair the cleft, as well as speech therapy and orthodontics. Surgical repair of the cleft lip is usually done at 3-9 months of age, while cleft palate repair is typically between 18-24 months. Non-surgical treatments like dental obturators may also be used. Nursing care focuses on safe feeding and preventing aspiration during intake.

















































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)

















