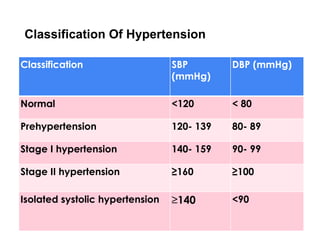
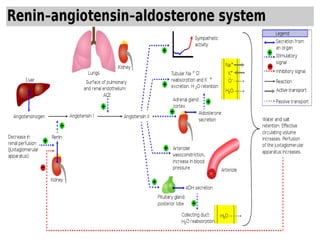
Hypertension, or high blood pressure, is a major risk factor for stroke and heart attacks. It is usually asymptomatic and requires regular screening. The document defines hypertension as a blood pressure reading over 140/90 mmHg. It classifies hypertension into stages and discusses essential (primary) hypertension, which makes up 95% of cases, versus secondary hypertension, which has an identifiable underlying cause such as kidney, heart, endocrine or neurological diseases. The document explores causes of essential hypertension like salt overload, activation of the renin-angiotensin-aldosterone system, and sympathetic nervous system activation. It also examines various secondary causes of hypertension.


![1- Salt/volume overload
● Salt (sodium chloride) overload/volume overload is
one of the common causes of hypertension.
● Essential hypertension has been associated with
high sodium intake in a variety of scientific models,
clinical studies and trials
● it is certified that decreasing the sodium intake
ameliorates this effect [40, 41].
● High sodium intake
❖ increases blood pressure by expanding
intravascular volume
❖ may have direct neurohormonal effects on the
cardiovascular system](https://image.slidesharecdn.com/med6hypertension-230316103920-60bf1208/85/MED-6-Hypertension-pdf-15-320.jpg)










































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
