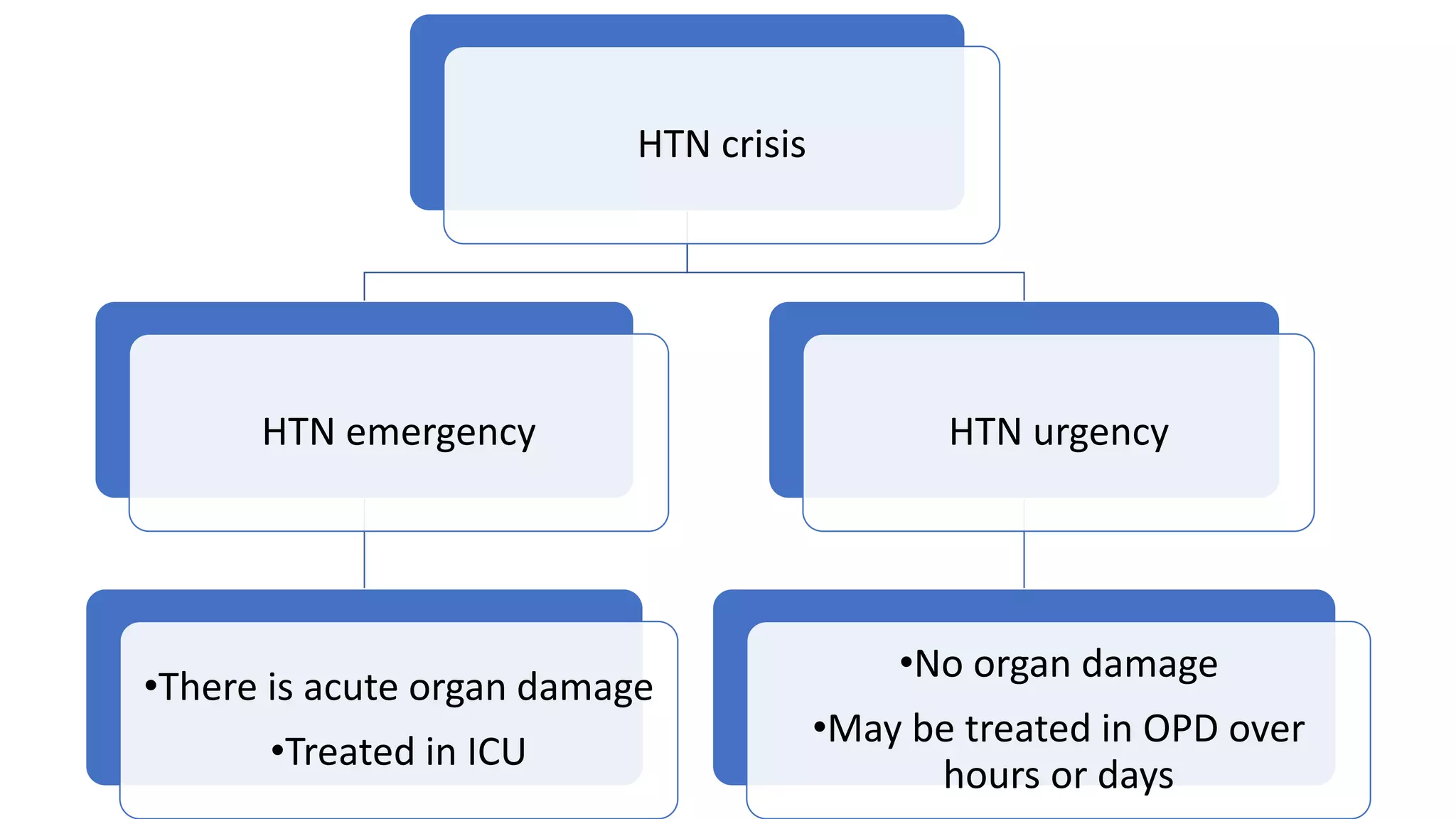
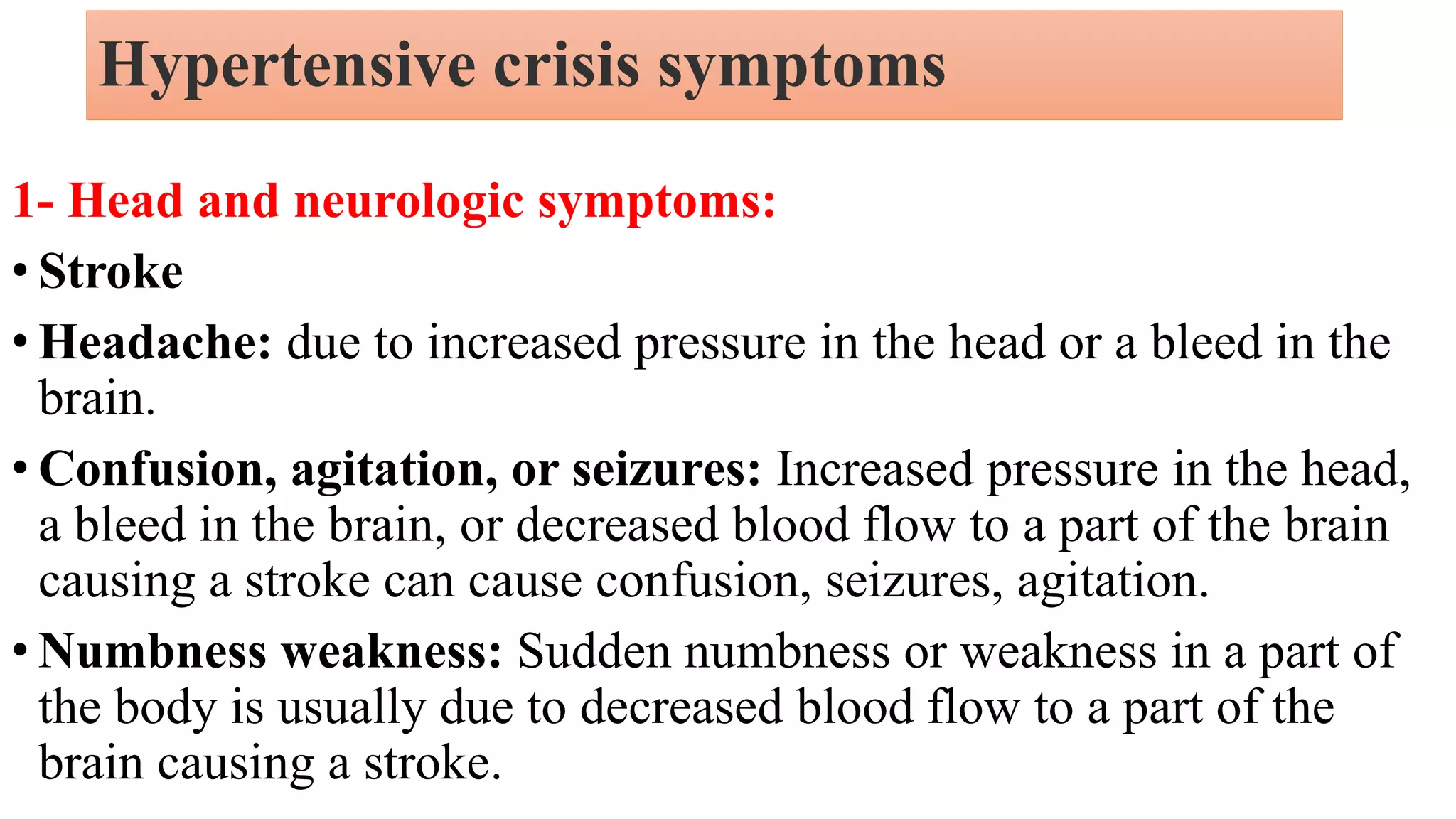
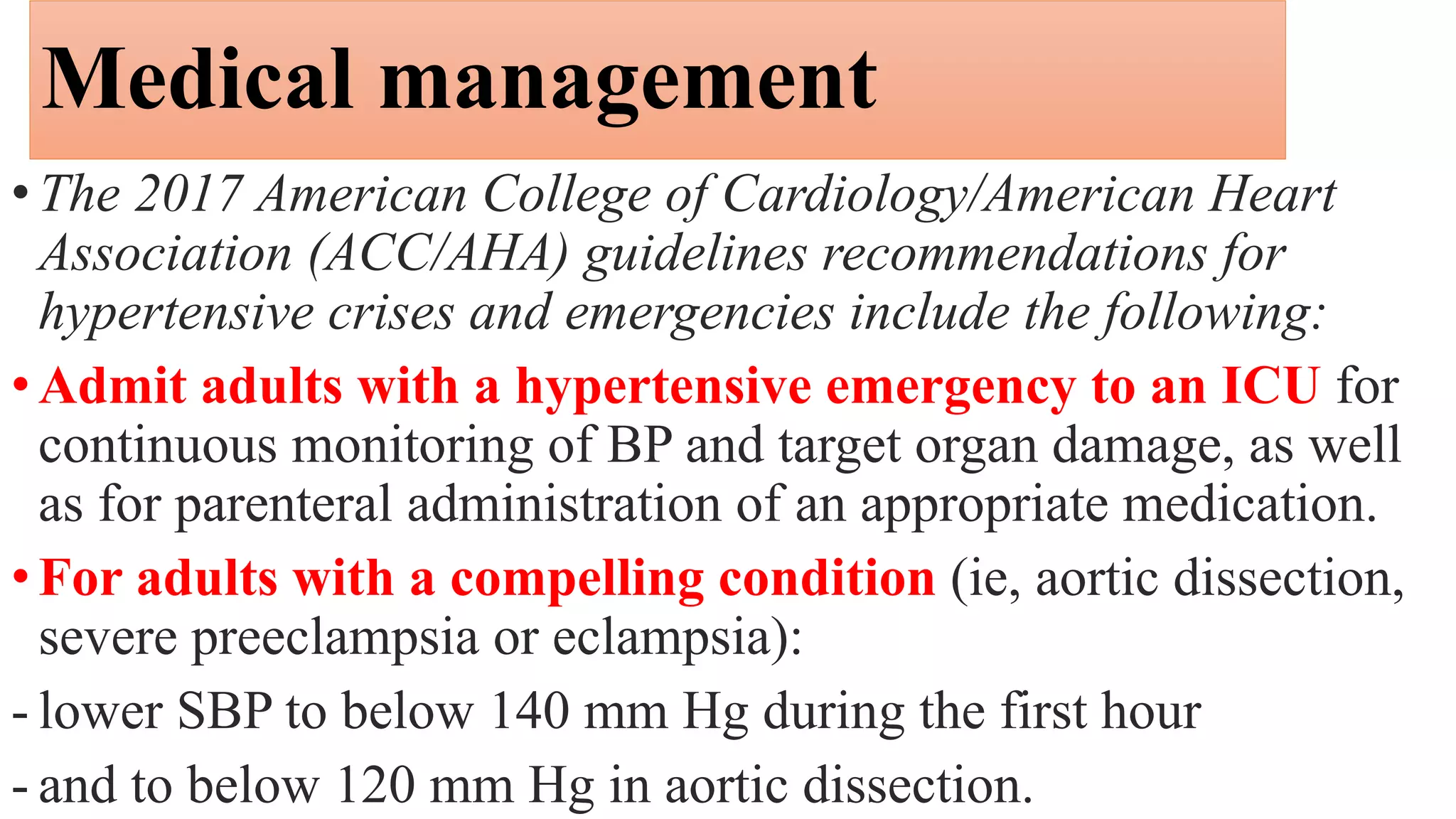
A hypertensive crisis is a sudden spike in blood pressure to 180/120 mmHg or higher, which is a medical emergency that could lead to organ damage or be life-threatening. Symptoms include headaches, confusion, chest pain, nausea, and weakness. Causes include non-compliance with medications, high salt/fat diets, certain drugs, kidney disease, and hormone imbalances. Treatment involves reducing blood pressure in the ICU over hours to days depending on any organ damage present. Nursing care focuses on monitoring, medication administration, lifestyle changes, and education to prevent future crises.