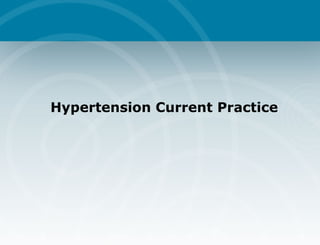
![Prevalence of Cardiovascular Disease 10 20 30 40 50 60 High BP CAD CHF Stroke Other 50,000,000 12,200,000 4,600,000 4,400,000 2,800,000 Prevalence (millions) BP=blood pressure, CAD=coronary artery disease, CHF=congestive heart failure Estimated Number of Persons With Cardiovascular Disease in the US ,[object Object],(24%)](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Hypertension+current
Similar to Hypertension+current (20)
More from dhavalshah4424
More from dhavalshah4424 (20)
Recently uploaded
Recently uploaded (20)
Hypertension+current
- 7. Hypertension: A Significant CV and Renal Disease Risk Factor National High Blood Pressure Education Program Working Group. Arch Intern Med. 1993;153:186-208.
- 8. CV Mortality Risk Doubles with Each 20/10 mm Hg BP Increment* *Individuals aged 40-69 years, starting at BP 115/75 mm Hg. CV, cardiovascular; SBP, systolic blood pressure; DBP, diastolic blood pressure Lewington S, et al. Lancet . 2002; 60:1903-1913. JNC VII. JAMA. 2003. CV mortality risk SBP/DBP (mm Hg) 0 1 2 3 4 5 6 7 8 115/75 135/85 155/95 175/105
- 11. BP Control Rates Trends in awareness, treatment, and control of high blood pressure in adults ages 18–74 Sources: Unpublished data for 1999–2000 computed by M. Wolz, National Heart, Lung, and Blood Institute; JNC 6. National Health and Nutrition Examination Survey, Percent II 1976–80 II (Phase 1) 1988–91 II (Phase 2) 1991–94 1999–2000 Awareness 51 73 68 70 Treatment 31 55 54 59 Control 10 29 27 34
- 12. Blood Pressure Classification JNC 7 Definition Hypertension 2003;42:1206-52 Blood Pressure (mm Hg) Category Systolic Diastolic <120 and <80 Normal 120-139 or 80-89 Prehypertension 140-159 or 90-99 Stage 1 hypertension ≥ 160 or ≥100 Stage 2 hypertension
- 13. "The Goal is to Get to Goal!” JNC VII recommended BP goals Hypertension -PLUS- Diabetes or Renal Disease < 140/90 mmHg < 130/80 mmHg
- 15. 4-Year Progression To Hypertension: The Framingham Heart Study (<120/80 mm Hg) (130/85 mm Hg) (130-139/85-89 mm Hg) Vasan, et al. Lancet 2001;358:1682-86 Participants age 36 and older
- 17. † CVD designation is determined by the constellation of risk factors, early disease markers, and target-organ disease. CVD, cardiovascular disease. ASH Writing Group Definition and Classification of Hypertension Classification Normal Stage 1 hypertension Stage 2 hypertension Stage 3 hypertension Descriptive Category Normal BP or rare blood pressure elevations AND No identifiable CVD † Occasional or intermittent BP elevations OR Early CVD † Sustained BP elevations OR Progressive CVD † Marked and sustained BP elevations OR Advanced CVD † Cardiovascular Risk Factors None or few Several Many Many Early Disease Markers None Usually present Overtly present Overtly present with progression Target-organ Disease None None Early signs present Overtly present with or without CVD events
- 20. BP Measurement Techniques http://hin.nhlbi.nih.gov/nhbpep_slds/menu.htm; Accessed October 20, 2003; 8:15AM Method Brief Description In-office Two readings, 5 minutes apart. Sitting in chair, not on exam table. Confirm elevated reading in contralateral arm. Self-measurement Provides information on response to therapy. May help improve adherence to therapy and evaluate “white-coat” HTN. Ambulatory BP monitoring Indicated for evaluation of “white-coat” HTN. Can be used to confirm self-measurement when inconsistent with in-office measurement. Reimbursable.
- 24. Impact of a 5 mmHg Reduction Hypertension 2003;289:2560-2572. Overall Reduction Stroke 14% Coronary Heart Disease 9% All Cause Mortality 7%
- 26. Management: JNC 7 GUIDELINES
- 27. Old Paradigm BP Cholesterol Disease Disease Treatment Treatment Normal Normal GOAL : Target Response
- 28. Current Paradigm DISEASE BP Cholesterol GOAL : Target Response TREATMENT
- 29. Classification and Management of BP for adults *Treatment determined by highest BP category. † Initial combined therapy should be used cautiously in those at risk for orthostatic hypotension. ‡ Treat patients with chronic kidney disease or diabetes to BP goal of <130/80 mmHg. BP classification SBP* mmHg DBP* mmHg Lifestyle modification Initial drug therapy Without compelling indication With compelling indications Normal <120 & <80 Encourage Prehypertension 120–139 or 80–89 Yes No antihypertensive drug indicated. Drug(s) for compelling indications. ‡ Stage 1 Hypertension 140–159 or 90–99 Yes Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Drug(s) for the compelling indications. ‡ Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) as needed. Stage 2 Hypertension > 160 or > 100 Yes Two-drug combination for most † (usually thiazide-type diuretic and ACEI or ARB or BB or CCB).
- 30. Anti Hypertensive drug classes The A, B, C, D approach
- 32. AB/CD Rule – HT Treatment AGE Younger (< 55) ACEi, Beta-blocker Ca++-blocker, Diuretic) (AB/CD = Dickerson et al. Lancet 353:2008-11;1999 Older (> 55) ACEi / ARB BB A + B A + B + D Diuretic CCB D + C + A D + C I II III III II I Resistant HT / Intolerance Add / substitute alpha blocker Re-consider 2 0 causes trial of spironolactone IV: V:
- 33. Compelling Indications for Individual Drug Classes Compelling Indication Initial Therapy Clinical Trial Basis ACC/AHA Heart Failure Guideline, MERIT-HF, COPERNICUS, CIBIS, SOLVD, AIRE, TRACE, ValHEFT, RALES ACC/AHA Post-MI Guideline, BHAT, SAVE, Capricorn, EPHESUS ALLHAT, HOPE, ANBP2, LIFE, CONVINCE THIAZ, BB, ACEI, ARB, ALDO ANT BB, ACEI, ALDO ANT THIAZ, BB, ACE, CCB Heart failure Post myocardial infarction High CAD risk
- 34. Compelling Indications for Individual Drug Classes Diabetes Chronic kidney disease Recurrent stroke prevention Compelling Indication Initial Therapy Options Clinical Trial Basis NKF-ADA Guideline, UKPDS, ALLHAT NKF Guideline, Captopril Trial, RENAAL, IDNT, REIN, AASK PROGRESS THIAZ, BB, ACE, ARB, CCB ACEI, ARB THIAZ, ACEI
- 37. Thank You
Editor's Notes
- 2 nd most common reason for visit All family physicians should be experts at HTN.
- Hypertension is an important contributing risk factor for morbidity and mortality from both cardiovascular (CV) and renal disease. Hypertension is one of the most significant contributing factors to the development of CV and renal disease. Complications of hypertension include coronary artery disease, congestive heart failure, stroke, renal disease (including end-stage renal disease), and peripheral vascular disease. These diseases account for significant disability, loss of productivity, and decreased quality of life for many Americans. National High Blood Pressure Education Program Working Group. National High Blood Pressure Education Program Working Group report on primary prevention of hypertension. Arch Intern Med. 1993;153:186-208.