Beyond mountains there are mountains (Haitian Proverb)
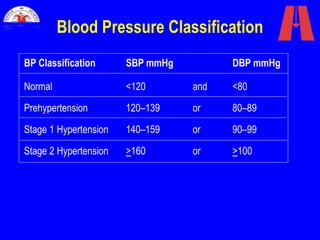
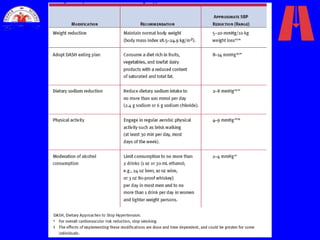
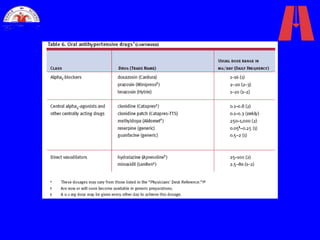
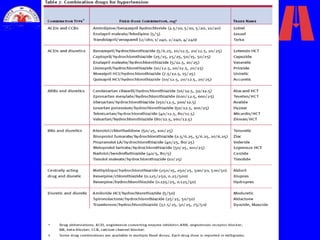
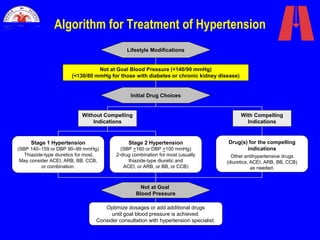
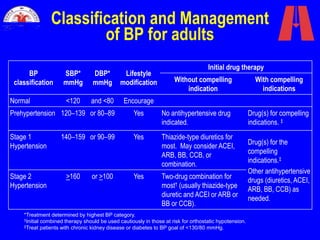
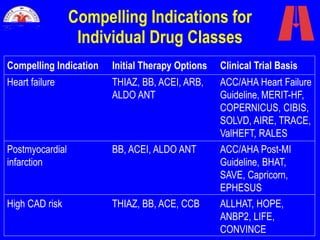
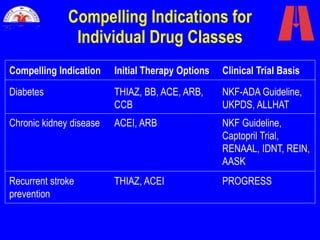
The document discusses guidelines for diagnosing and treating hypertension from the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). It outlines classifications for normal blood pressure and stages of hypertension based on systolic and diastolic readings. It also provides recommendations on lifestyle modifications, drug therapies, treatment goals, and monitoring for hypertensive patients.




































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




