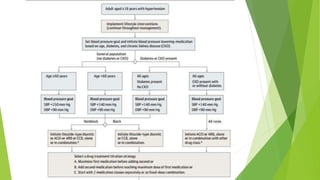
This document summarizes guidelines from the Eighth Joint National Committee (JNC 8) on the prevention, detection, evaluation, and treatment of high blood pressure. It provides recommendations on when to initiate pharmacologic treatment based on age, race, presence of diabetes or chronic kidney disease. It recommends treating to a blood pressure goal of less than 150/90 mmHg for those aged 60 or older, and less than 140/90 mmHg for others. It also provides guidance on first-line antihypertensive drug classes based on patient characteristics.








![“Statements and recommendations for [BP]
treatment based on a systematic review of
the literature to meet user needs, especially
the needs of the primary care clinician.”](https://image.slidesharecdn.com/final-160121164226/85/Hypertension-Guidelines-JNC-8-12-320.jpg)

![Age Recommendations, JNC 2014
• 18 years old and younger: Not considered
• 30 years old and younger: We have little to no data
• 30 to 59 years old: In the general population younger than 60 years, initiate
pharmacologic treatment to lower BP at a DBP of 90 mm Hg and treat to a
goal DBP lower than 90 mm Hg. Strong Recommendation: Grade A
• 60 years old: In the general population aged 60 years or older, initiate
pharmacologic treatment to lower BP at an SBP of 150 mm Hg or higher or a
DBP of 90 mm Hg or higher and treat to a goal SBP lower than 150 mm Hg
and goal DBP lower than 90 mm Hg. Strong Recommendation: Grade A
• 80 years old: Based on HYVET*
*Hypertensions in very elderly Trial
James PA, et al. JAMA. 2014;311:507-520.[1]](https://image.slidesharecdn.com/final-160121164226/85/Hypertension-Guidelines-JNC-8-14-320.jpg)
![JNC Panel Recommendation for Patients With
Diabetes and Hypertension
• In the population aged 18 years and older with
diabetes, initiate pharmacologic treatment to
lower BP at an SBP of 140 mm Hg or a DBP of 90
mm Hg and treat to a goal of SBP lower than 140
mm Hg and goal DBP lower than 90 mm Hg. Expert
Opinion: Grade E
James PA, et al. JAMA. 2014;311:507-520.[1]](https://image.slidesharecdn.com/final-160121164226/85/Hypertension-Guidelines-JNC-8-15-320.jpg)
![JNC Panel Recommendation for Patients With
CKD
• In the population aged 18 years with CKD,
initiate pharmacologic treatment to lower BP
at an SBP of 140 mm Hg or a DBP of 90 mm
Hg and treat to goal of an SBP lower than 140
mm Hg and a goal DBP lower than 90 mm Hg.
Expert Opinion: Grade E
James PA, et al. JAMA. 2014;311:507-520.[1]](https://image.slidesharecdn.com/final-160121164226/85/Hypertension-Guidelines-JNC-8-16-320.jpg)
![JNC Recommendation for Nonblack Patients
• In the general nonblack population, including
those with diabetes, initial antihypertensive
treatment should include
– Thiazide-type diuretic
– Calcium channel blocker (CCB)
– Angiotensin-converting enzyme (ACE) inhibitor
– Angiotensin receptor blocker (ARB)
– Moderate Recommendation: Grade B
James PA, et al. JAMA. 2014;311:507-520.[1]](https://image.slidesharecdn.com/final-160121164226/85/Hypertension-Guidelines-JNC-8-17-320.jpg)
![JNC Recommendation for Black Patients
• In the general black population, including
those with diabetes, initial antihypertensive
treatment should include
– Thiazide-type diuretic
– CCB
• For the general black population:
– Moderate Recommendation: Grade B
• For black patients with diabetes:
– Weak Recommendation: Grade C
James PA, et al. JAMA. 2014;311:507-520.[1]](https://image.slidesharecdn.com/final-160121164226/85/Hypertension-Guidelines-JNC-8-18-320.jpg)
![James PA, et al. JAMA. 2014;311:507-520.[1]
Recommendations for Hypertension
Management
Recommendation 1: In the general population aged 60 years,
initiate pharmacologic treatment to lower BP at systolic BP
(SBP)150 mm Hg or diastolic BP (DBP) 90 mm Hg and treat to a
goal SBP lower than 150 mm Hg and goal DBP lower than 90 mm
Hg. (Strong Recommendation : Grade A)
Corollary Recommendation: In the general population aged 60
years, if pharmacologic treatment for high BP results in lower
achieved SBP (eg, <140 mm Hg) and treatment is well tolerated
and without adverse effects on health or quality of life, treatment
does not need to be adjusted. (Expert Opinion : Grade E)](https://image.slidesharecdn.com/final-160121164226/85/Hypertension-Guidelines-JNC-8-19-320.jpg)



![James PA, et al. JAMA. 2014;311:507-520.[1]
Recommendation 6: In the general nonblack population, including
those with diabetes, initial antihypertensive treatment should
include a thiazide-type diuretic, CCB, angiotensin-converting
enzyme inhibitor (ACEI), or angiotensin receptor blocker (ARB).
(Moderate Recommendation: Grade B)
Recommendations for Hypertension
Management](https://image.slidesharecdn.com/final-160121164226/85/Hypertension-Guidelines-JNC-8-24-320.jpg)

![Strategies for Reaching BP Goal
James PA, et al. JAMA. 2014;311:507-520.[1]
Start 1 drug, titrate to maximum dose, and
then add a second drug
Start 1 drug and then add a second drug before
achieving maximum dose of the initial drug
Begin with 2 drugs at the same time either as
2 separate pills or as a single pill combination](https://image.slidesharecdn.com/final-160121164226/85/Hypertension-Guidelines-JNC-8-27-320.jpg)



![References (cont)
11. Wright JT Jr, Harris-Haywood S, Pressel S, et al. Clinical outcomes by race in
hypertensive patients with and without the metabolic syndrome: Antihypertensive
and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Arch Intern
Med. 2008;168:207-217.
12. Wright Jr JT, Fine LJ, Lackland DT, Ogedegbe G, Dennison Himmelfarb CR.
Evidence Supporting a Systolic Blood Pressure Goal of Less Than 150 mm Hg in
Patients Aged 60 Years or Older: The Minority View. Ann Intern Med. 2014. [Epub
ahead of print]
13. Dahlöf B, Devereux RB, Kjeldsen SE, et al; LIFE Study Group. Cardiovascular
morbidity and mortality in the Losartan Intervention For Endpoint reduction in
hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359:995-
1003.
14. Poulter NR, Wedel H, Dahlöf B, et al; ASCOT Investigators. Role of blood
pressure and other variables in the differential cardiovascular event rates noted in
the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-
BPLA). Lancet. 2005;366:907-913.](https://image.slidesharecdn.com/final-160121164226/85/Hypertension-Guidelines-JNC-8-33-320.jpg)