Download as PDF, PPTX



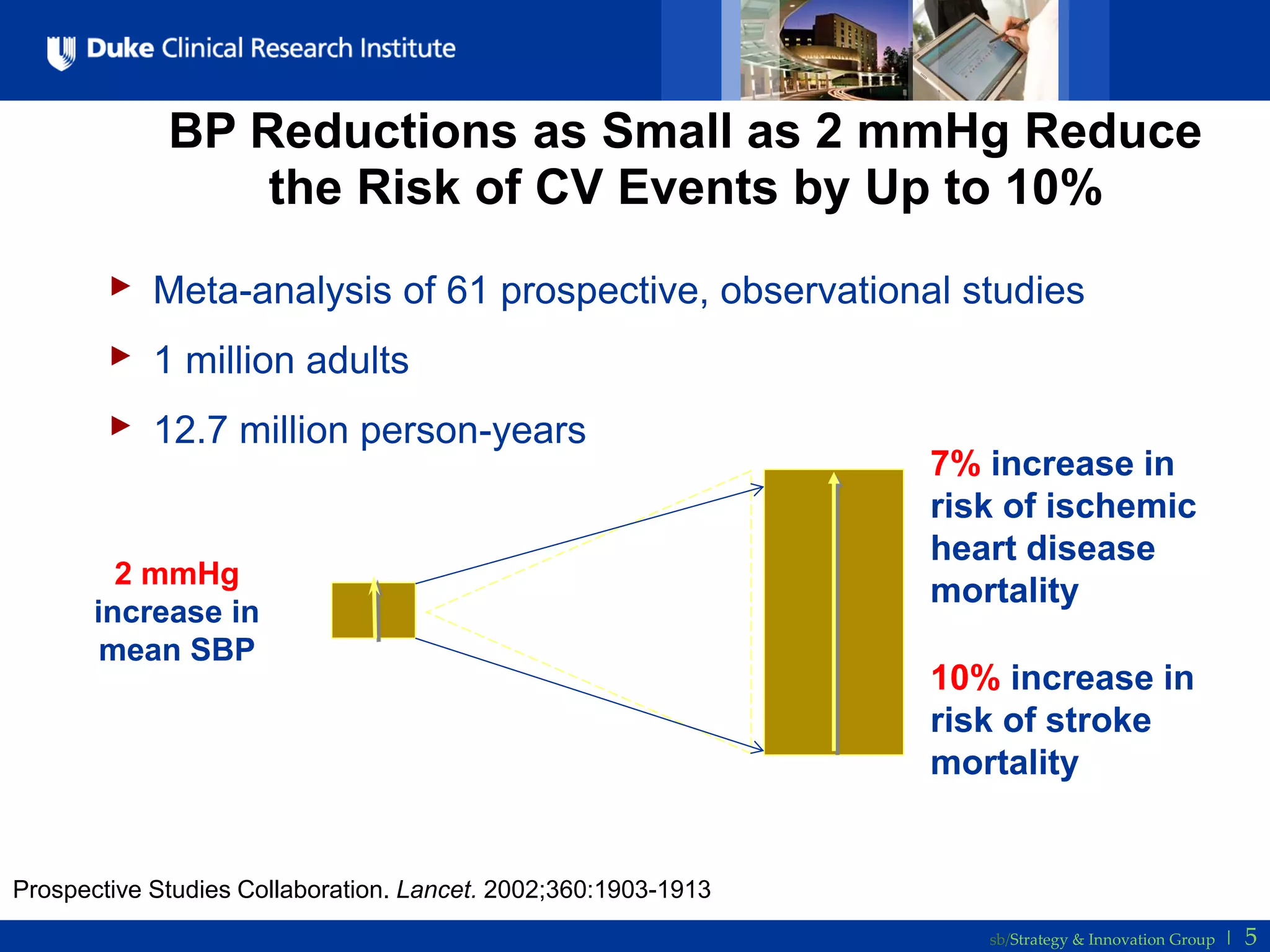
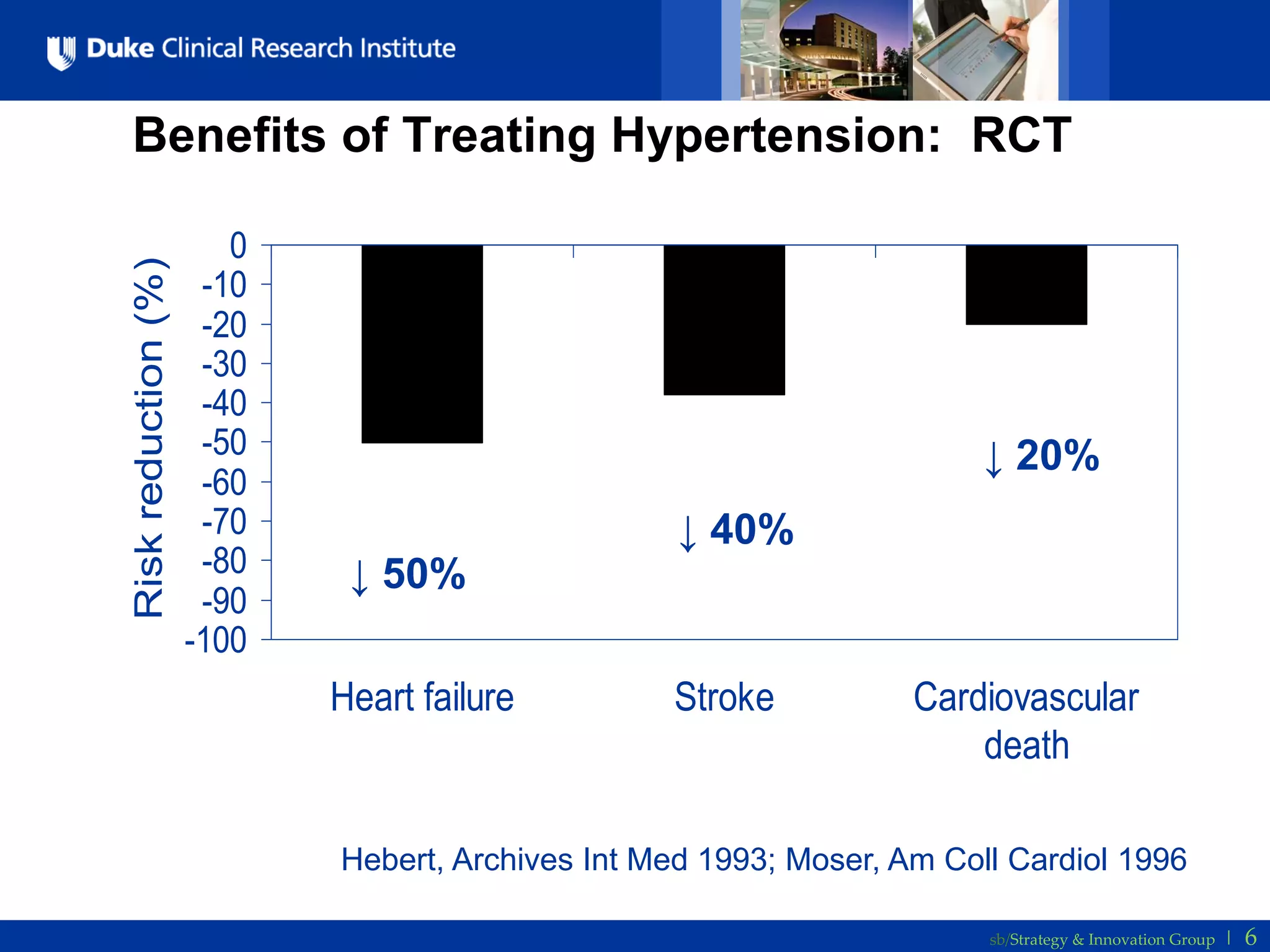
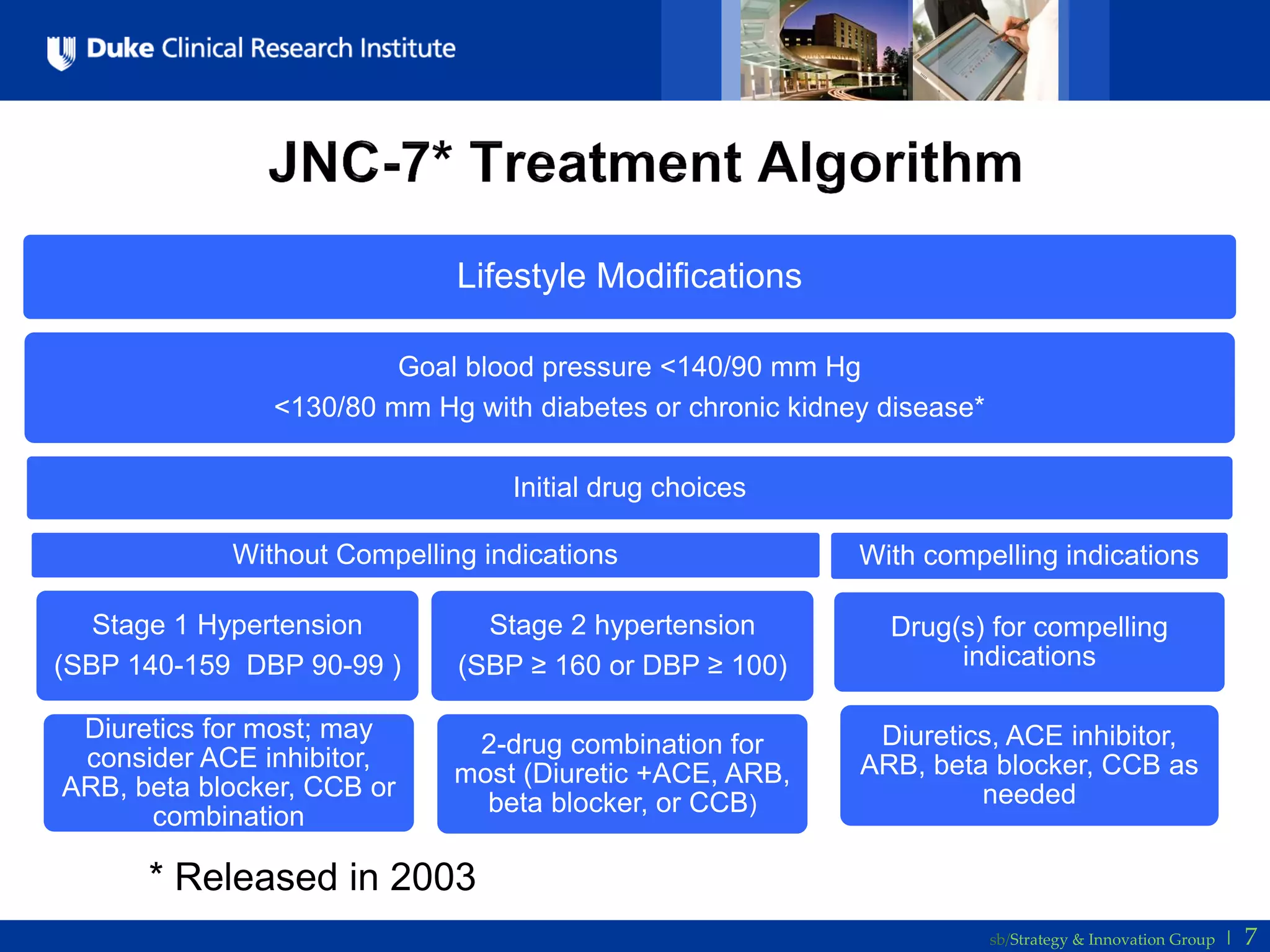


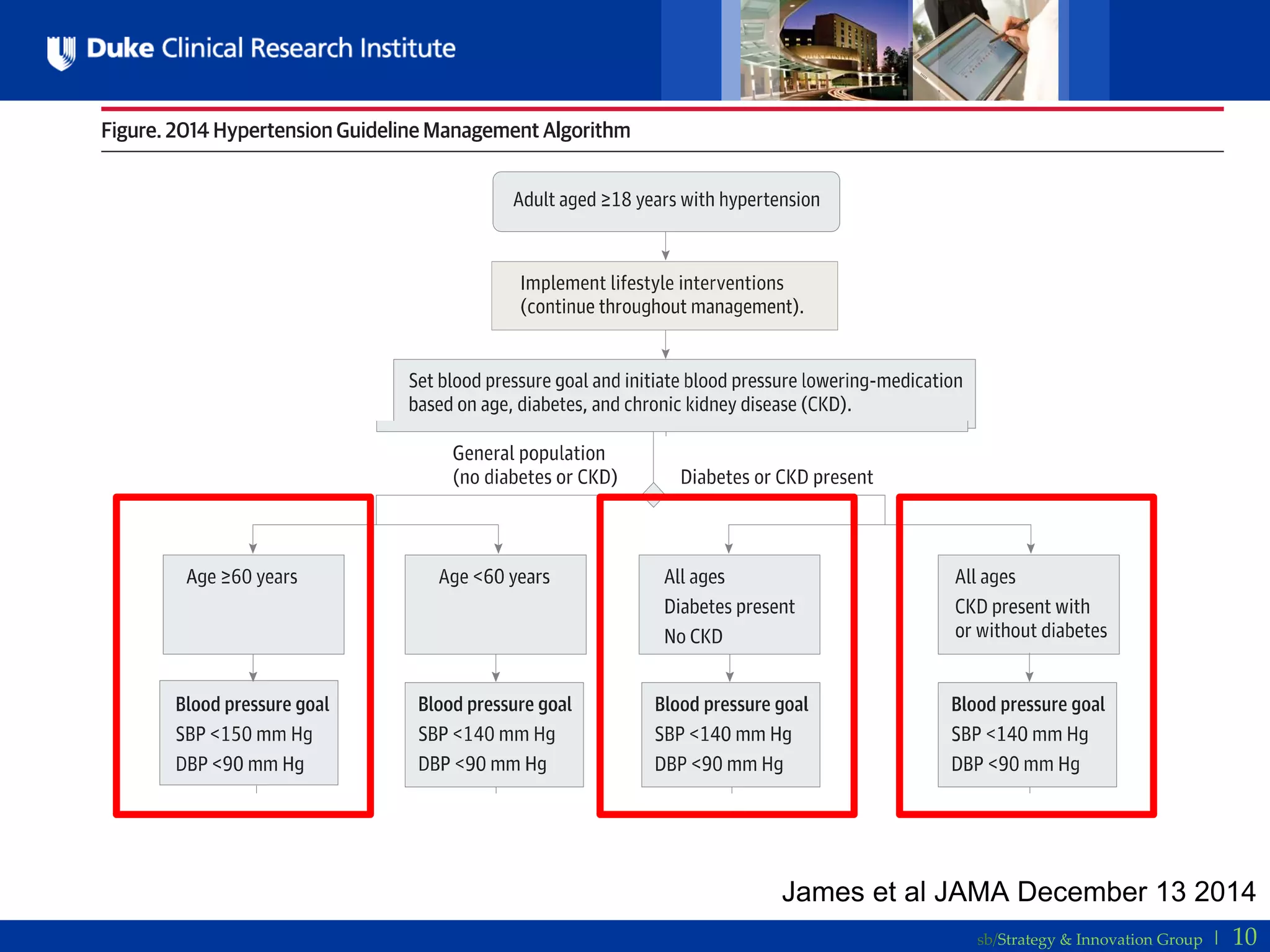
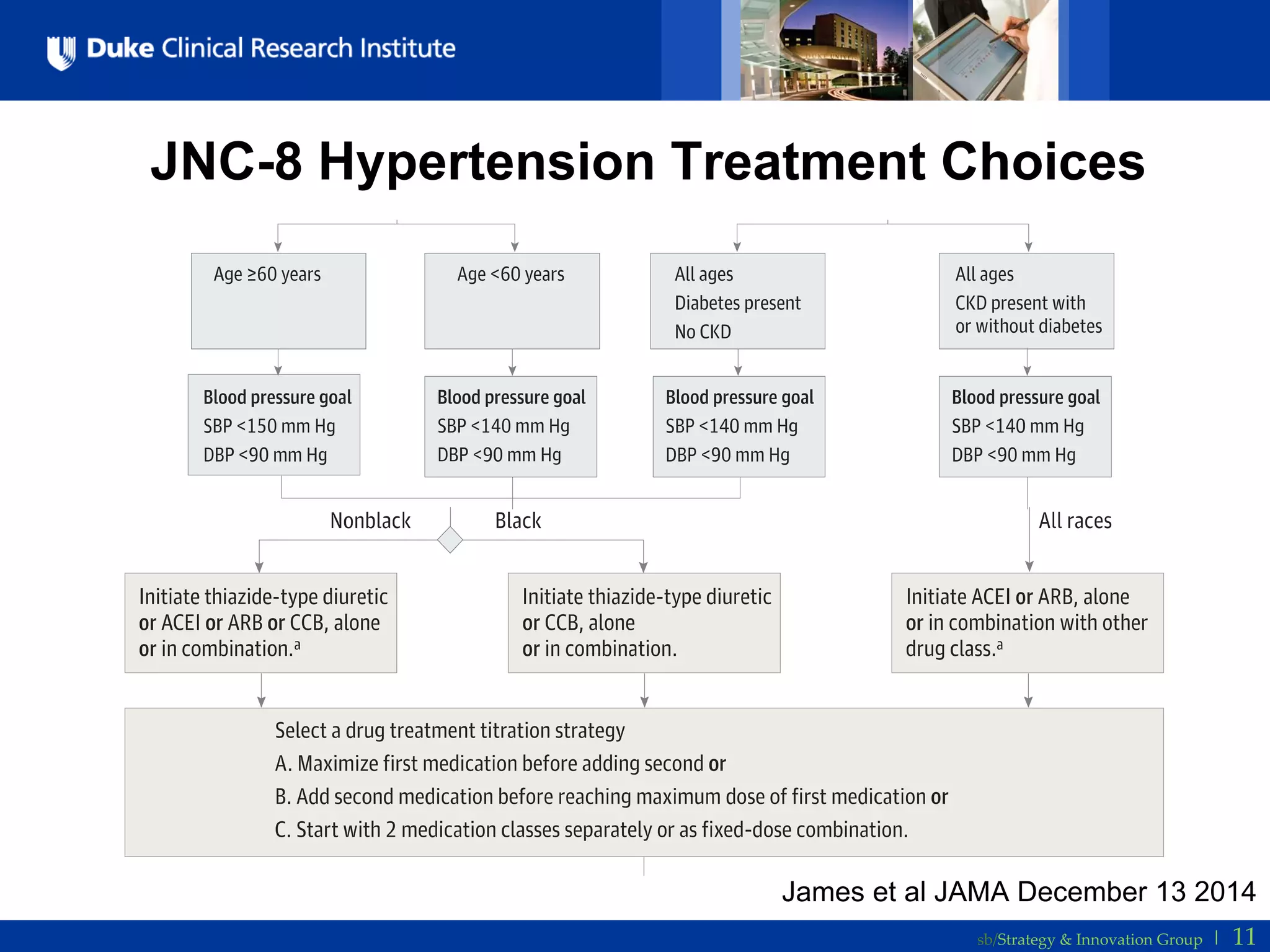
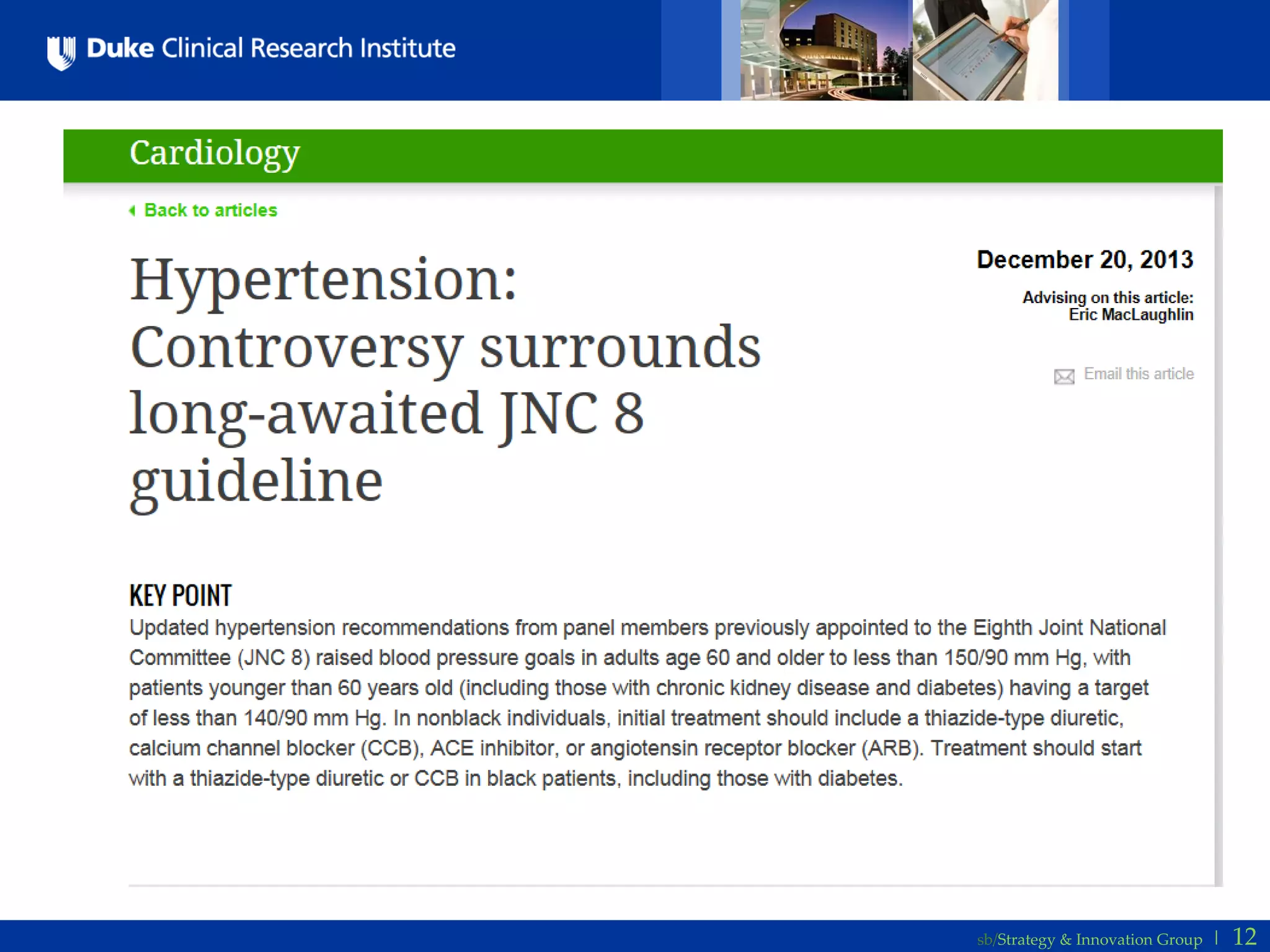








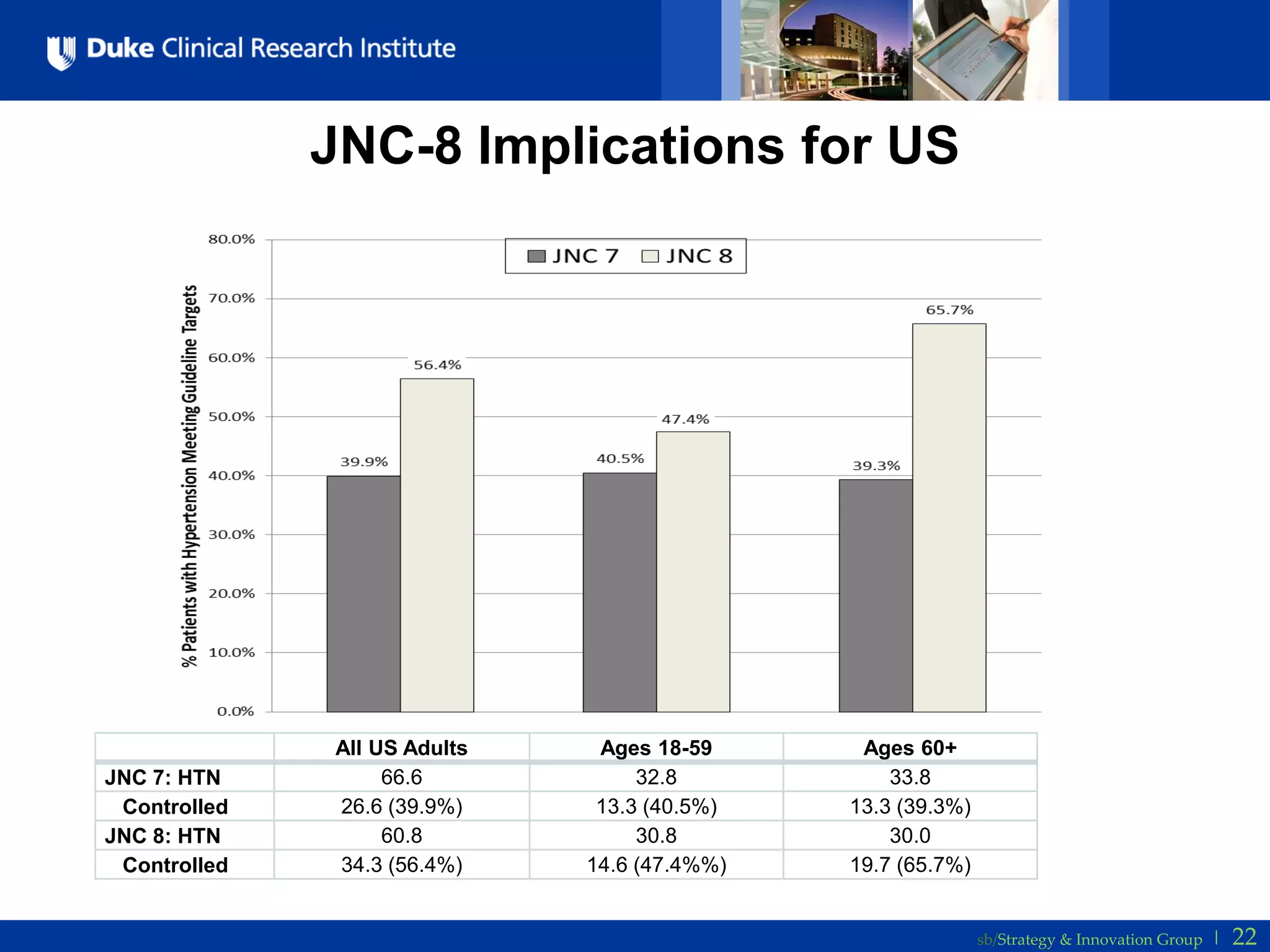



The document discusses the new JNC-8 guidelines for hypertension treatment. It provides background on hypertension prevalence, risks, and controversies in treatment approaches over time. It then summarizes the key aspects of the new JNC-8 guidelines, including less aggressive blood pressure targets for those over age 60 (150/90 mmHg vs. the previous 140/90 mmHg for all adults) based on a review of existing studies. The implications are that the new guidelines would reclassify a significant portion of older adults in the US as having their blood pressure under control.























































































