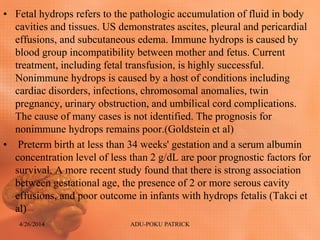
Download as PDF, PPTX



![Reference
s
Davis BE, Daley CM, Shurtleff DB, Duguay S, Seidel K, Loeser
JD, et al. Long-term survival of individuals with
myelomeningocele. Pediatr Neurosurg. Jul-Aug 2005;41(4):186-
91. [Medline].
Hagen-Ansert, S. L. (2012). Textbook of diagnostic sonography 7th
edition.
Vinchon M, Rekate HL, Kulkarni AV. Pediatric hydrocephalus
outcomes: a review. Fluids Barriers CNS. Aug 27 2012;9(1):18.
[Medline].
Rumack. (2011). Diagnostic ultrasound 4th edition.
Bullen PJ, Rankin JM, Robson SC: Investigation of the
epidemiology and prenatal diagnosis of holoprosencephaly in the
North of England, Am J Obstet Gynecol 184:1256-1262, 2001
Goldstein R. A practical approach to fetal chest masses.
Ultrasound Q 2006;22:177–19426.
Takci S, Gharibzadeh M, Yurdakok M, Ozyuncu O, Korkmaz A,
Akcoren Z, et al. Etiology and Outcome of Hydrops Fetalis: Report
of 62 Cases. Pediatr Neonatol. Oct 1 2013;[Medline].
4/26/2014 ADU-POKU PATRICK](https://image.slidesharecdn.com/hydrocephaluswithfetalhydrops-140523112513-phpapp02/85/Hydrocephalus-with-fetal-hydrops-40-320.jpg)

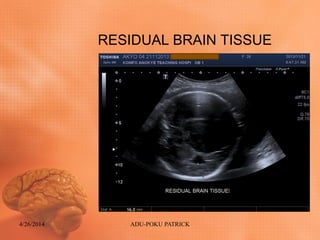
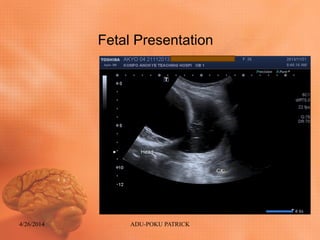
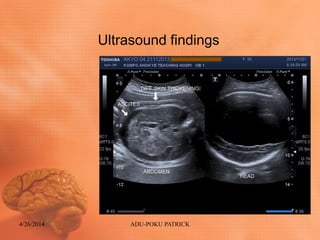
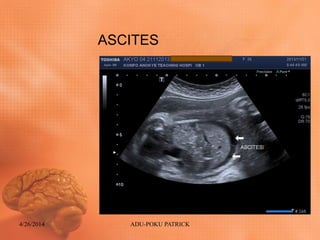
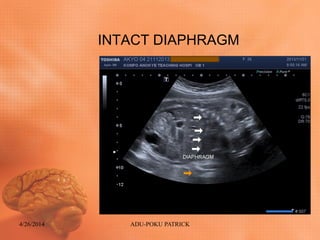
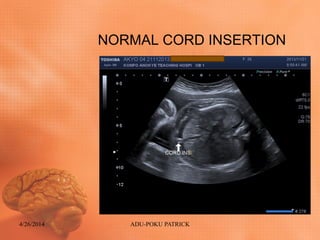
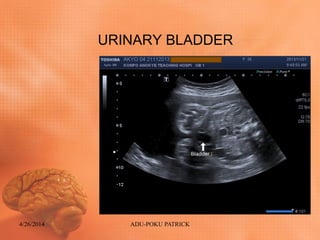
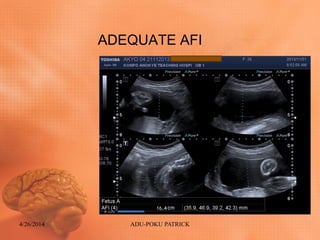
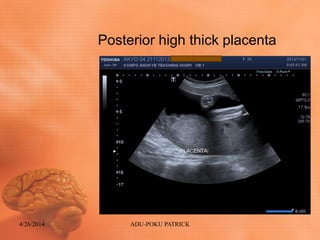
This document summarizes a clinical case presentation of a 26-year-old pregnant woman with hydrocephalus and fetal hydrops. An ultrasound found extensive cerebral spinal fluid collection in the fetus, indicating severe hydrocephalus. Additional findings of diffuse skin thickening, ascites, cardiomegaly, and edema suggested fetal hydrops. The fetus was in a cephalic presentation with normal anatomy elsewhere. After counseling, the woman opted for termination by cesarean section, which was performed and revealed an intrauterine fetal demise.