Downloaded 1,730 times







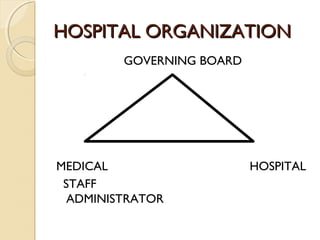

This document discusses the organizational structures of hospitals. It describes the classifications of healthcare as primary, secondary, and tertiary care. Hospitals are also classified as general, specialty, rehabilitation, long-term care, or nursing homes. Regulatory agencies oversee hospitals. The roles of the governing board, hospital administrator, and medical staff are outlined. Advances in technology have increased complexity and professional specialization within hospitals. Effective communication and leadership are needed to coordinate the diverse professionals and administrative functions within this complex organizational system.






![Organizational Structure Of A Hospital[1]](https://cdn.slidesharecdn.com/ss_thumbnails/organizationalstructureofahospital1-100104091259-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
























































































