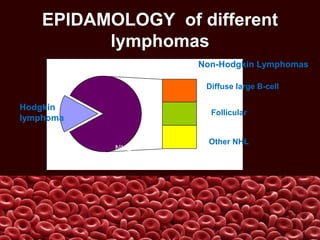
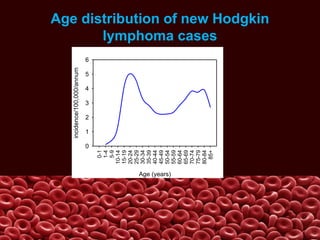
The document discusses hematologic disorders, focusing on lymphomas. It defines lymphomas as neoplasms of lymphoid cells that usually start in lymph nodes but can spread to other lymphatic tissues. Lymphomas are broadly classified into Hodgkin lymphoma and non-Hodgkin lymphoma (NHL). Hodgkin lymphoma is described in more detail, including its epidemiology, pathophysiology involving Reed-Sternberg cells, clinical manifestations, diagnostic criteria, medical management using chemotherapy and radiation, and nursing considerations around screening and education. NHL is discussed as a heterogeneous group of cancers involving malignant B or T lymphocytes that can infiltrate multiple lymph node sites and extranodal tissues.































































![animated slideshowpp [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/animatedslideshowppautosaved-230815193818-406bcb84-thumbnail.jpg?width=640&height=640&fit=bounds)



























