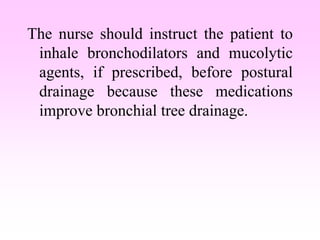
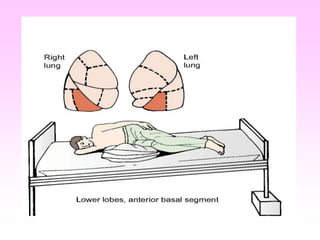
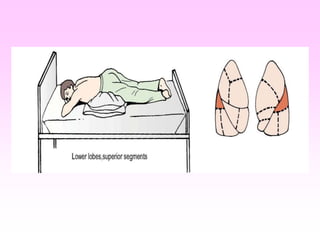
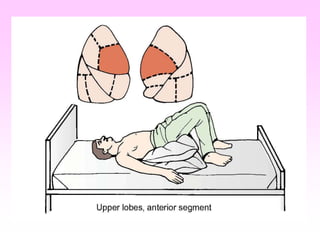
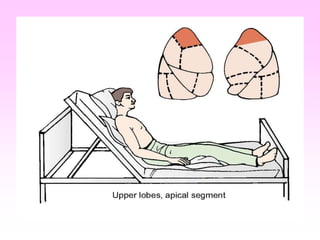
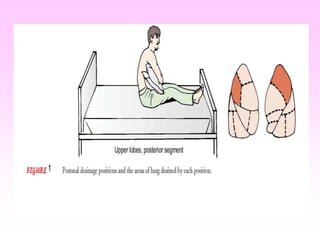
This document describes respiratory care modalities including chest physiotherapy techniques like postural drainage, percussion, and breathing exercises. Postural drainage uses specific positions and gravity to drain secretions from the lungs into the trachea where they can be coughed or suctioned out. Percussion helps loosen thick secretions for removal. Breathing retraining teaches pursed-lip breathing and diaphragmatic breathing to make breathing more efficient. The nurse's role is to instruct patients and families on these techniques and ensure they are performed correctly and safely to clear the lungs and improve ventilation.
































































![animated slideshowpp [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/animatedslideshowppautosaved-230815193818-406bcb84-thumbnail.jpg?width=640&height=640&fit=bounds)



























