Chronic osteomyelitis is difficult to treat and eradicate completely. It is characterized by infected dead bone within soft tissue with poor blood supply, making systemic antibiotics ineffective. Surgical debridement of infected bone and soft tissue is usually required along with long-term antibiotics. Eliminating dead space after debridement can be challenging and may require bone grafting, antibiotic beads, or flaps to fill gaps and promote healing.














![TREATMENT
Supportive treatment .
● Antibiotics – to prevent spread.
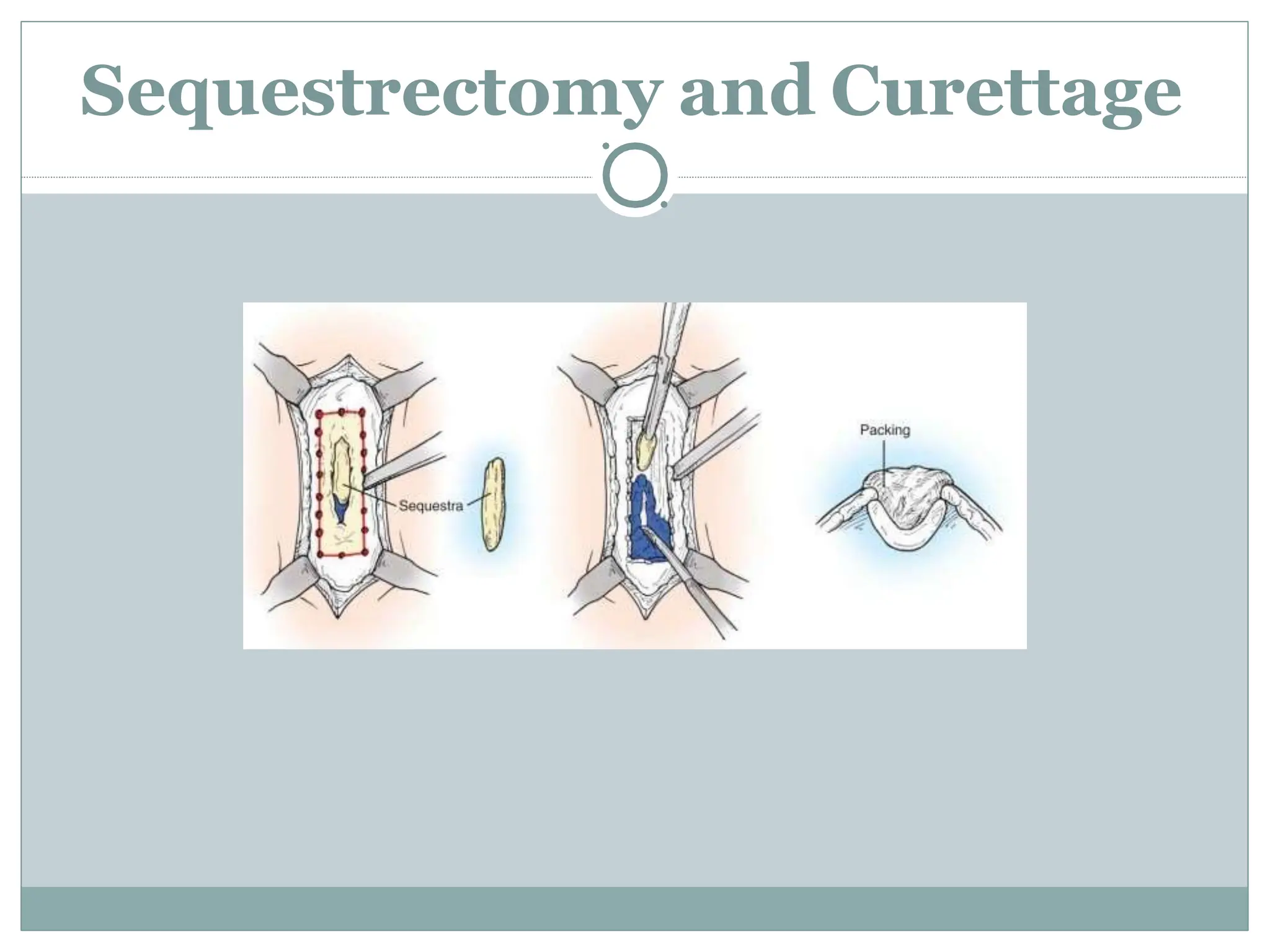
● Surgery – sequestretomy + saucerization
[cannot be eradicated without surgical intervention]](https://image.slidesharecdn.com/chronicosteomyelitispowerpt-240328122714-b27c029f/75/chronicosteomyelitis-Powerpt-power-point-16-2048.jpg)









































![Overview of Fungal Infections[1].ppt pptx](https://cdn.slidesharecdn.com/ss_thumbnails/overviewoffungalinfections1-250811070114-3c4fbad5-thumbnail.jpg?width=640&height=640&fit=bounds)




![Gas gangrene [Autosaved].pptxGas gangrene [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gasgangreneautosaved-250608063811-c85a18a4-thumbnail.jpg?width=640&height=640&fit=bounds)





























