Download as PDF, PPTX



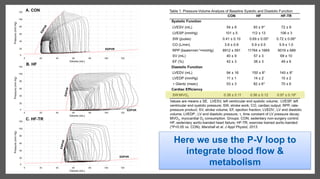
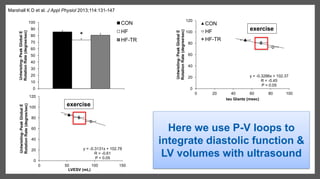
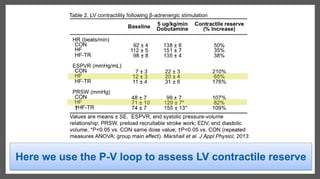
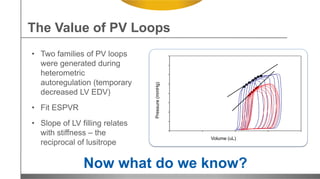
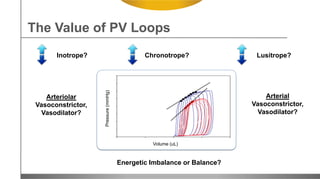
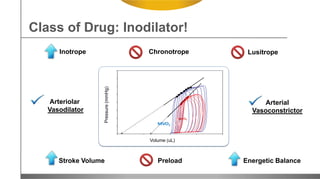


1. PV loops provide a comprehensive examination of cardiac function by integrating measurements of pressures, volumes, flows, and metabolism. 2. The presenter uses PV loops in mini-pigs to evaluate the impacts of exercise and pharmacological therapies on heart failure with preserved ejection fraction. 3. PV loops allow the integration of data from multiple methodologies to assess global cardiovascular function and the effects of treatments. The presenter is planning to next examine different exercise intensities and combinations with therapies.























































































