Downloaded 13 times






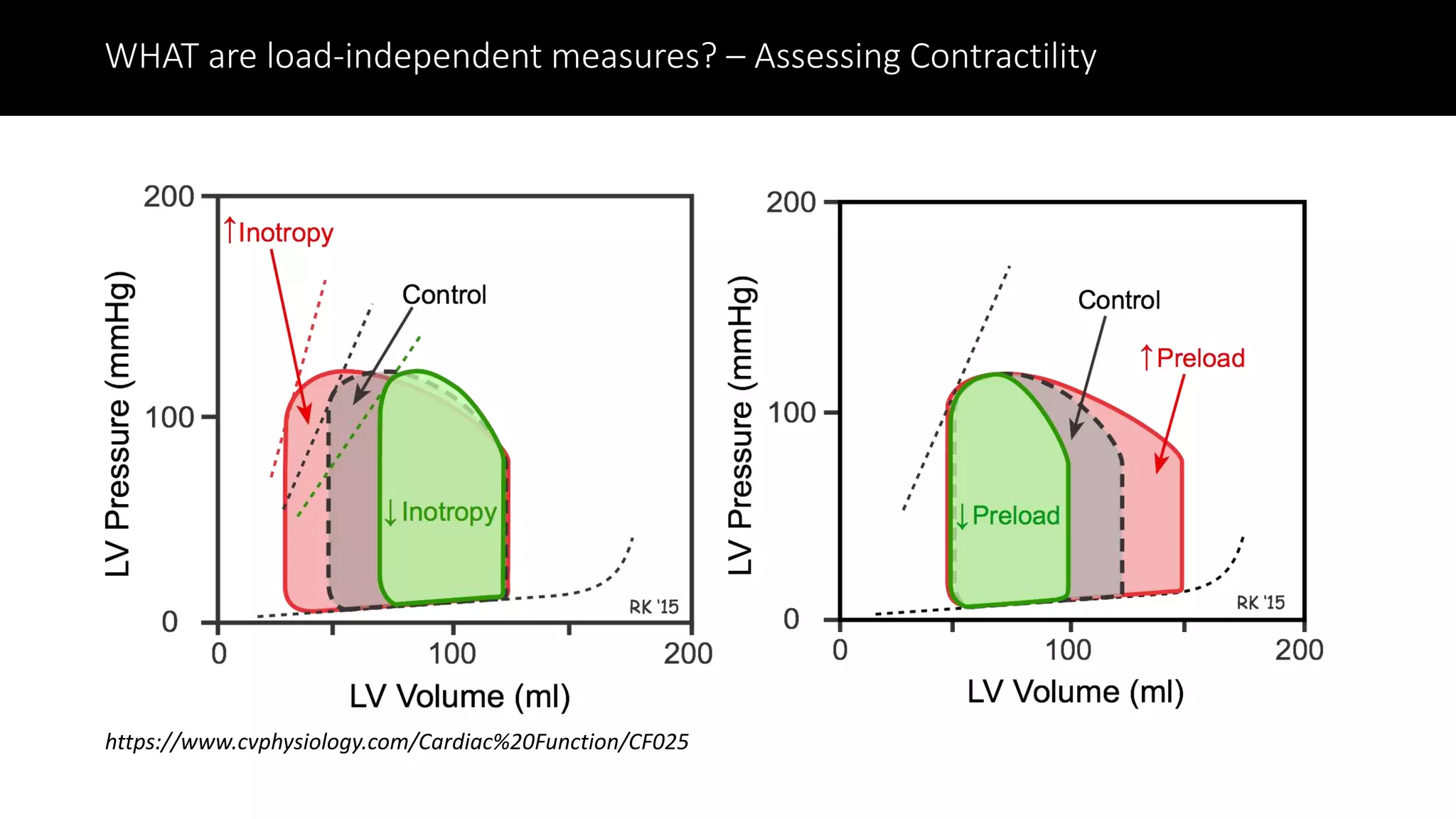
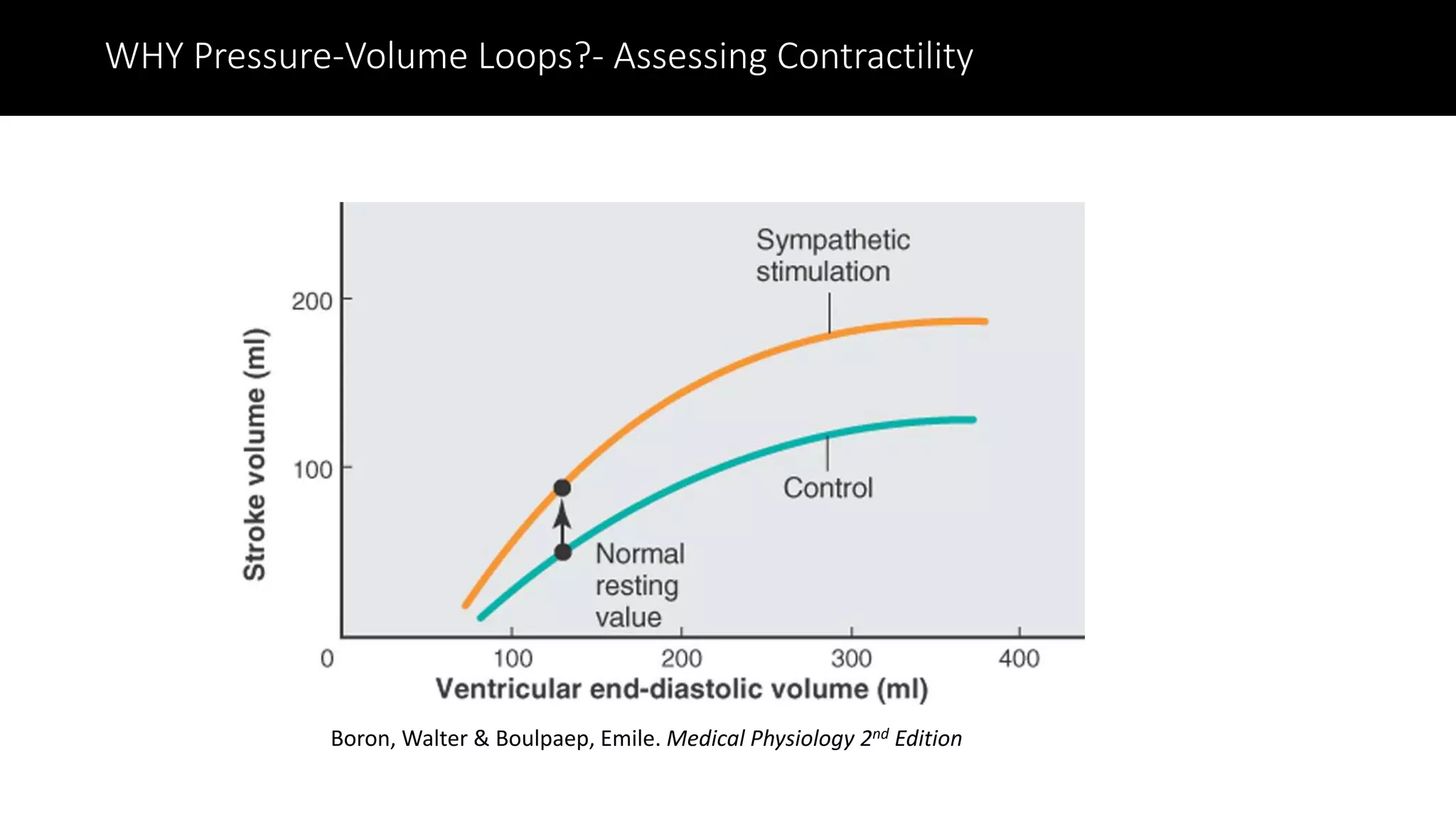





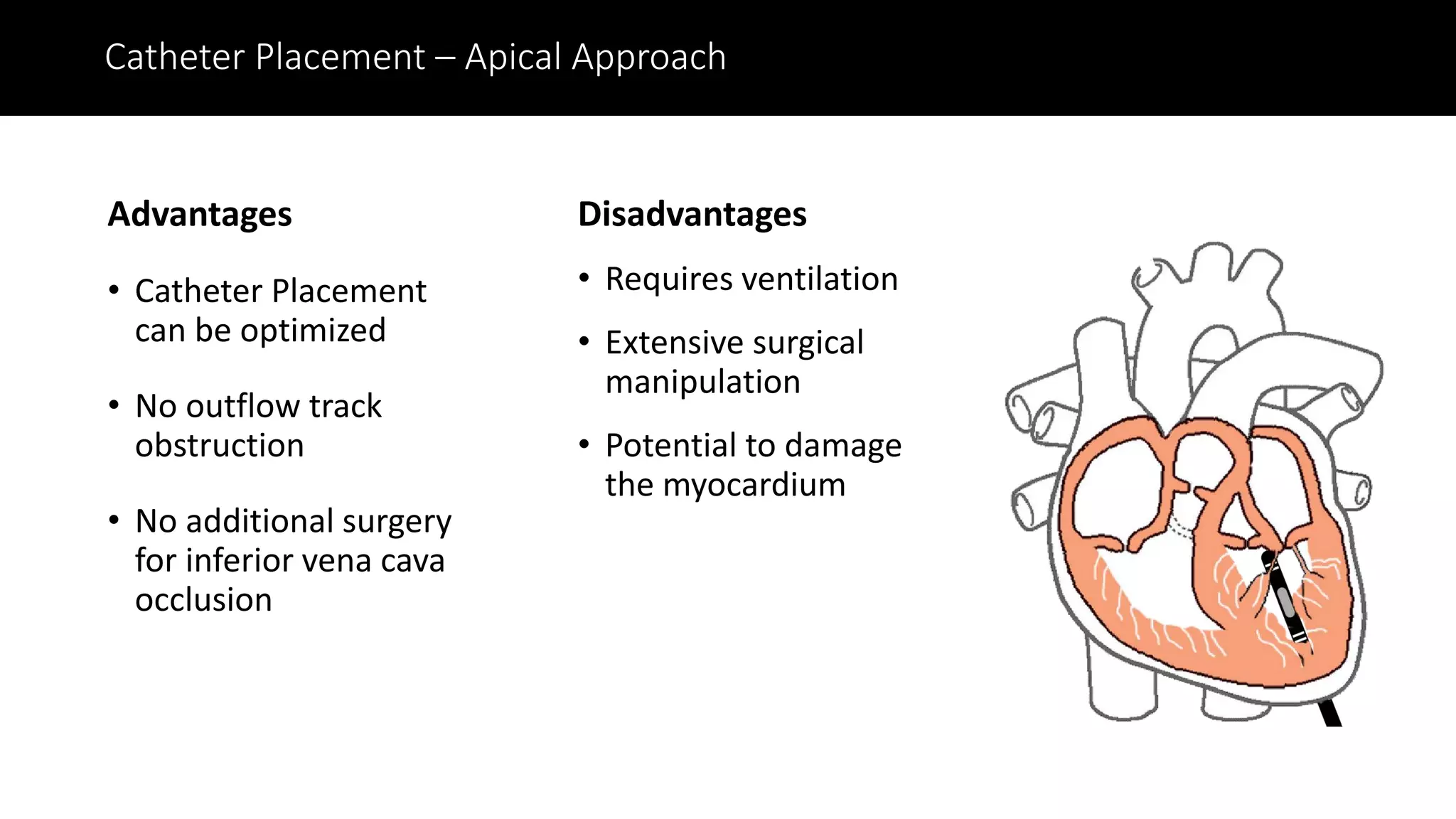




The document outlines the fundamentals of cardiac pressure-volume loop analysis as a means to evaluate cardiac function, presented by Dr. Dewayne Townsend and Dr. Adam Goodwill. It discusses the advantages and limitations of pressure-volume loop methodologies, as well as various measures of cardiac performance and contractility. Additionally, it addresses the technical considerations and challenges associated with obtaining accurate pressure-volume loop data in research settings.























































































