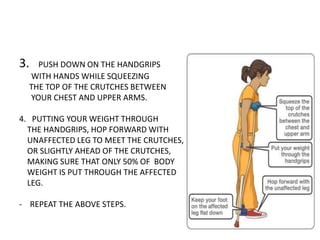
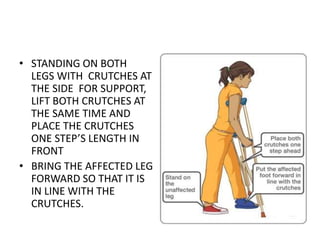
This document provides instructions for non-weight bearing and partial weight bearing walking using crutches after lower limb fractures. It discusses the importance of early mobility to avoid complications of prolonged bed rest and promote healing. Complications from prolonged bed rest that affect various body systems are described. Detailed instructions are provided for different types of crutch walking including non-weight bearing, touch down weight bearing, and partial weight bearing. Measurements for proper crutch fitting and instructions for using crutches to climb and descend stairs are also outlined.